StraightSmile Solutions®
What Is the “Airway Trifecta” in Phase 1 Interceptive Orthodontics?
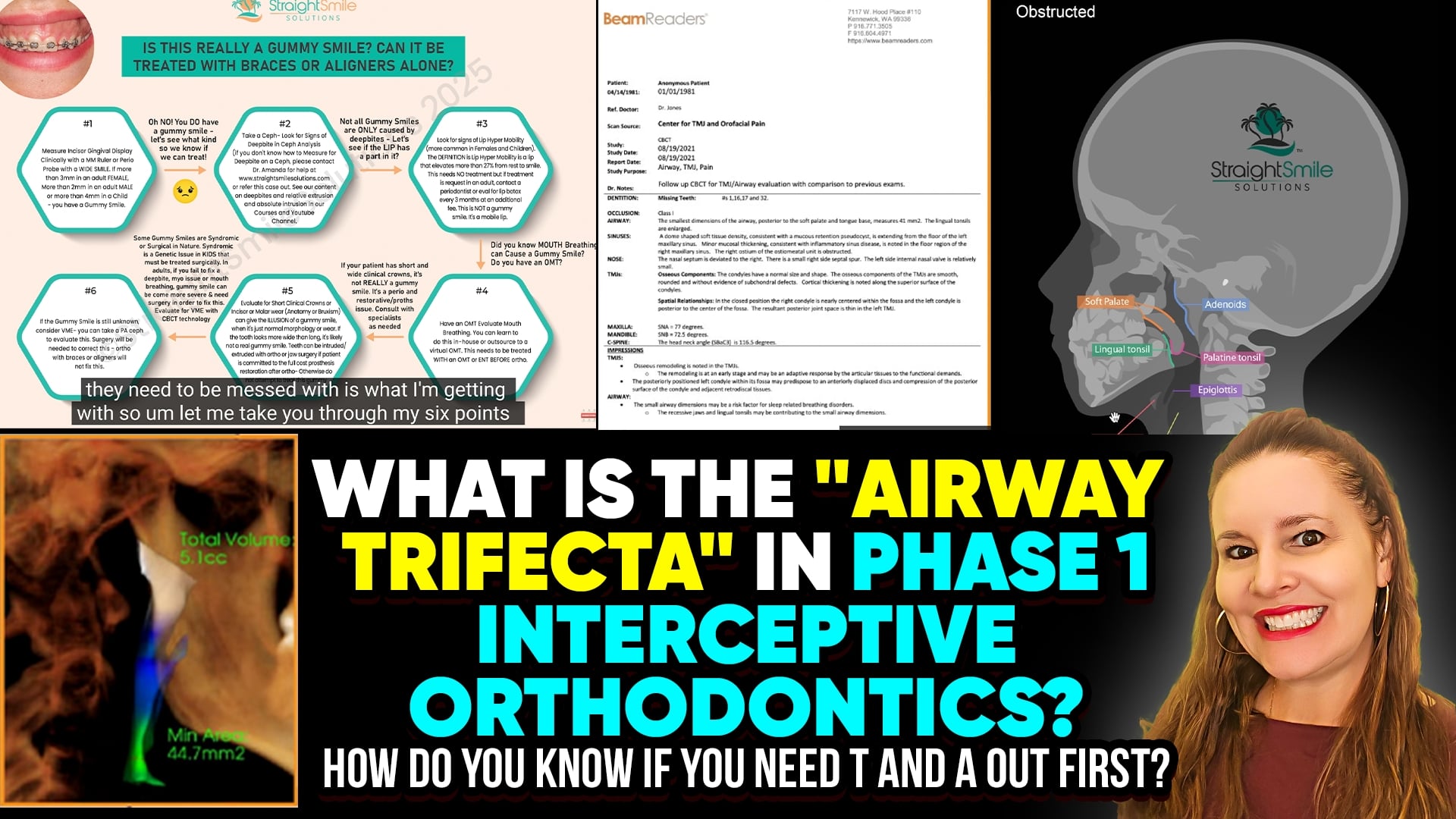
I. Introduction
Dr. Amanda from Straight Smile Solutions explains a structured approach to evaluating airway health in Phase 1 interceptive orthodontic patients.
The focus is on proper screening before orthodontic treatment, especially in children.
She emphasizes that jumping straight into orthodontics without airway evaluation can worsen outcomes.
The concept of the “Airway Trifecta” highlights the most critical red flags that must be assessed first.
II. Airway Trifecta and Comprehensive Screening
Subjective Screening
Use structured questionnaires completed at home, not in the office.
Parents should observe the child’s sleep over multiple nights.
Video recordings of breathing or sleep disturbances are strongly encouraged.
Watch for snoring, mouth breathing, restless sleep, and pauses in breathing.
Daytime Behavioral and Physical Red Flags
Chronic mouth breathing observed in the waiting room.
Daytime sleepiness or fatigue.
ADHD-like behaviors and poor focus (correlation, not causation).
Nocturnal enuresis (bedwetting).
Dark circles under the eyes.
“Airway face” characteristics.
Objective Clinical Screening
Long facial growth patterns.
Narrow arches and vertically excessive growth.
Gummy smiles linked to airway dysfunction.
Small or constricted airways seen on lateral ceph or CBCT.
Radiology reports suggesting potential airway compromise.
Myofunctional (Myio) Screening
In-office screening by the orthodontist is essential.
Identification of tongue posture issues, swallowing dysfunction, and oral habits.
Referral to a myofunctional therapist when multiple red flags are present.
Recognition that myofunctional therapy is time-intensive and specialized.
Interdisciplinary Referrals
ENT evaluation when tonsils, adenoids, or nasal obstruction are suspected.
Myofunctional therapy before orthodontics when habits persist.
Avoid initiating orthodontics until airway, habits, and obstruction are addressed.
Treatment Planning Across All Planes of Space
Expansion alone is often insufficient.
Consider sagittal (AP), vertical, and transverse discrepancies.
Jaw positioning and bite correction may be required.
Untreated airway or habit issues increase relapse risk.
III. Conclusion
The “Airway Trifecta” reinforces the importance of thorough subjective and objective screening, myofunctional evaluation, and interdisciplinary collaboration before Phase 1 orthodontic treatment. Addressing airway health first protects both the patient and provider, reduces relapse, and leads to more stable, functional outcomes. Knowing when to delay treatment and refer is a sign of responsible, airway-centered orthodontic care.
Do Sleep Appliances or ARS (Anterior Repositioning Splints) Cause TMD to the TMJ and Bite Relapse?
Introduction
Dr. Amanda addresses a growing clinical trend she is seeing more frequently: patients presenting with unexplained bite shifts, orthodontic relapse, and TMJ symptoms linked to sleep appliances and anterior repositioning splints. Many of these devices are prescribed without clear communication about their potential joint, bite, and long-term risks, raising both clinical and liability concerns.
Key Clinical Concerns with Sleep Appliances and ARS
- Mandibular Advancement Devices (MADs)
- Commonly prescribed for sleep apnea
- Can cause jaw soreness, joint tenderness, and TMD
- Apply prolonged forward positioning forces on the mandible
- Stretch TMJ ligaments, which are not visible on CBCT (MRI required)
- FDA alerts have noted long-term joint and bite complications with some jaw remodeling devices
- Anterior Repositioning Splints (ARS)
- Designed to temporarily recapture the TMJ disc
- May reduce clicking and pain short term
- Use beyond ~6 weeks can contribute to permanent joint damage
- Joint inflammation or ligament injury may go undetected on standard imaging
- Orthodontic Bite Changes
- Posterior open bites are the most common complication
- Anterior-only contacts and occlusal instability
- Dental tipping, spacing, and relapse that may not be fully correctable
- Continuous force application causes bite “drift,” even in adults
- Patient Education and Liability
- Patients are often warned about bite changes but not joint damage
- Long-term pain, dysfunction, or surgical needs may develop
- Inadequate informed consent increases future legal risk
- Why Dr. Amanda Avoids This Space
- These devices do not address underlying skeletal problems
- Interceptive orthodontics in children is safer and preventive
- Early jaw development reduces future sleep-related complications
Conclusion
Sleep appliances and anterior repositioning splints are not benign. While they may be necessary in select cases, they carry real risks to the TMJ and occlusion, especially when prescribed without full disclosure. Dr. Amanda emphasizes the importance of caution, thorough documentation, and patient education while advocating for early interceptive orthodontics as the safest long-term solution.
Are LLHA (Lower Lingual Holding Arches) Dangerous? Do You Need Them If You Pull C’s or D’s?
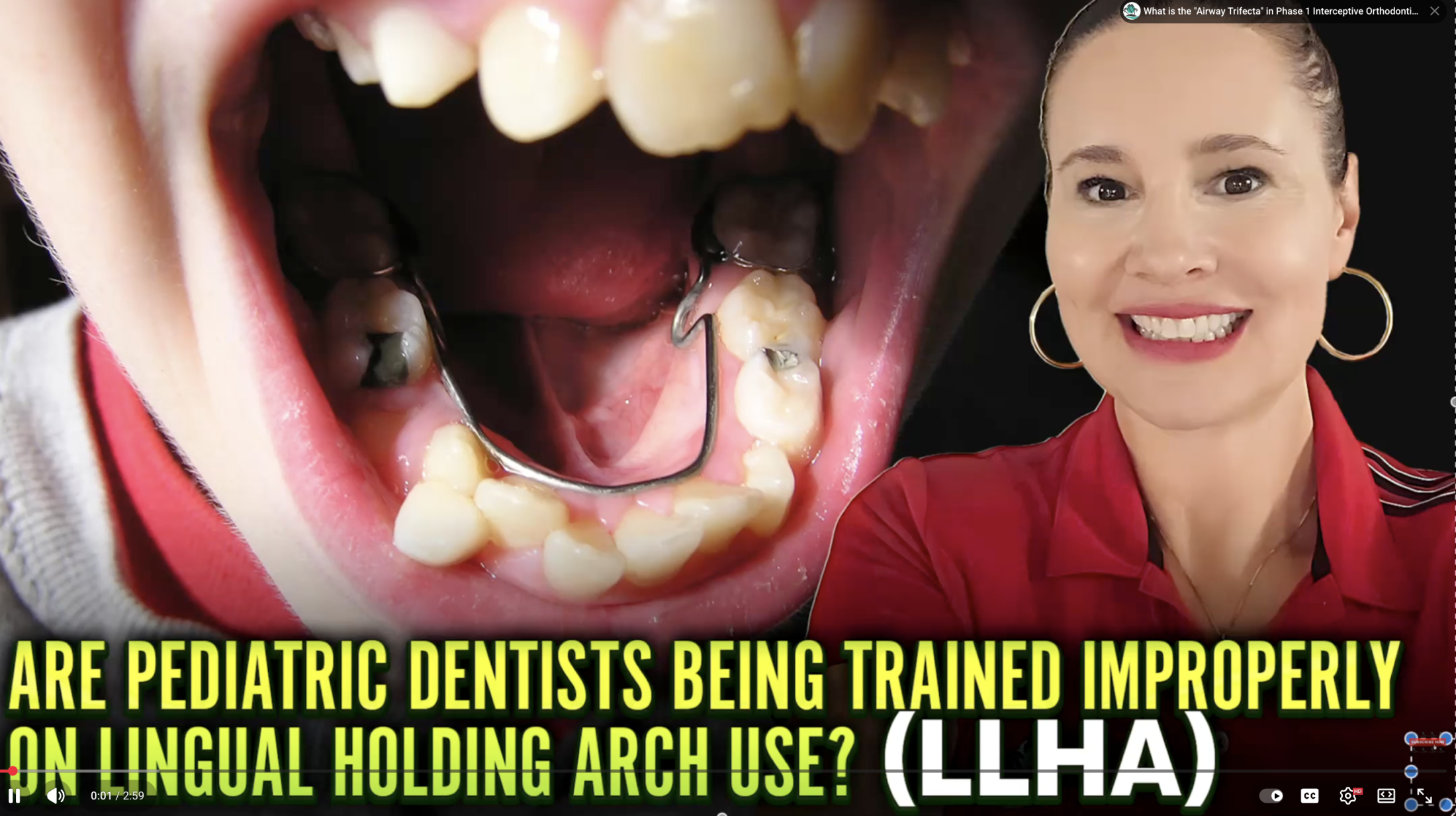
Are LLHA (Lower Lingual Holding Arches) Dangerous? Do You Need Them If You Pull C’s or D’s?
I. Introduction
Dr. Amanda from Straight Smile Solutions addresses common myths and the overuse of Lower Lingual Holding Arches (LLHAs). LLHAs are widely used by orthodontists and pediatric dentists for anchorage and space maintenance. While they have valid indications, Dr. Amanda cautions that they are often placed automatically and unnecessarily, especially after extracting primary canines (C’s) or first primary molars (D’s).
II. What LLHAs Are Actually Meant to Do
- Designed for:
- Space maintenance
- Anchorage control
- Most appropriate when:
- A primary second molar (E) is lost early
- The permanent second premolar (5) is not erupting soon
- They are not meant to be routine appliances placed after every lower primary extraction.
III. The Myth: You Must Place an LLHA After Pulling C’s or D’s
- According to orthodontic literature and residency training:
- From age 6–7 and up, LLHAs are not routinely required after removing C’s or D’s.
- Pulling a single lower canine:
- May theoretically cause a midline shift
- Dr. Amanda’s preference: remove the contralateral canine instead of placing an LLHA.
- Pulling a D:
- Rarely causes space loss when the E is still present.
- Lower teeth do not migrate significantly, especially with developing premolars underneath.
IV. The Incisor Retroclination Myth
- Claim: Lower incisors will retrocline if an LLHA is not placed.
- Reality:
- Incisor movement does not occur without orthodontic forces.
- Any relapse after Phase 1 orthodontics is a retention issue, not caused by extracting baby teeth.
- Retroclined incisors without ortho usually indicate:
- Myofunctional problems
- Muscle imbalance
- A lingual arch will not fix these issues.
V. When LLHAs Are Appropriate
- After early loss of a primary E (unless the 5 is erupting soon).
- In select cases with:
- Mild Class III tendencies
- Established arch development
- Never place an LLHA on:
- An undeveloped, constricted arch
- A poor bite that hasn’t been corrected first.
Conclusion
LLHAs are valuable when used correctly, but harmful when overused. Dr. Amanda estimates that 90% of LLHAs placed are unnecessary, and 10% actively worsen the bite. Clinicians should abandon the use of automatic appliance placement and instead rely on proper diagnosis, arch development, and evidence-based orthodontic principles to avoid doing more harm than good.
How to Vertically Integrate a DSO to Launch or Scale Orthodontics Even with Staff Turnover
Introduction
Dr. Amanda from Straight Smile Solutions discusses how DSOs can successfully launch or scale their orthodontic practices. The focus is on achieving cost-effective and sustainable growth across multiple locations. Special emphasis is placed on pediatric and multi-site DSOs with frequent staff or doctor turnover. Vertical integration, not aligner engines or outsourced AI, is presented as the safest and most profitable model.
The Core Problem DSOs Face
- High provider and staff turnover disrupts orthodontic continuity.
- Relying on a single orthodontist or external aligner “engine” creates instability.
- AI-driven treatment planning does not teach doctors how to diagnose or plan cases.
- Patient transfers and doctor exits expose gaps in decentralized systems.
Why Vertical Integration Works
- Centralizes orthodontic decision-making and workflows.
- Allows the “show to run from the top,” not from individual providers.
- Protects cases when doctors leave or patients move between locations.
- Creates consistency across dozens of offices.
Building a Vertically Integrated Ortho System
- Start with data collection:
- Most DSOs already have scanners and are using them.
- Train teams to consistently take scans and records.
- Implement front-end screening:
- One centralized team reviews cases first.
- Viable cases are identified before doctor involvement.
- Distribute cases through:
- Interested doctors with guided support, or
- Study clubs (weekly, monthly, or biweekly).
Study Clubs Over One-on-One Consulting
- More scalable and cost-effective for large DSOs.
- Support collaborative treatment planning.
- Reduce reliance on expensive per-doctor consulting.
- Allow systems to be refined and repeated across locations.
Training the Entire Team
- Everyone should know how to:
- Take scans
- Collect orthodontic records
- Manage check-in and follow-up workflows
- Avoid bottlenecks by eliminating single-role dependency.
Ownership, Incentives, and KPIs
- Appoint an internal ortho lead or ortho maven.
- Offer KPI-based bonuses to encourage ownership.
- Rockstar TCs, RDAs, or OMs can successfully lead programs.
- Incentivized leadership drives consistency and growth.
Conclusion
Vertical integration enables DSOs to scale orthodontics ethically, profitably, and predictably, even in the face of staff turnover. By leveraging existing scanners, centralized screening, study clubs, and team-wide training, DSOs can avoid costly AI shortcuts and build repeatable systems that prioritize patient outcomes and long-term success.
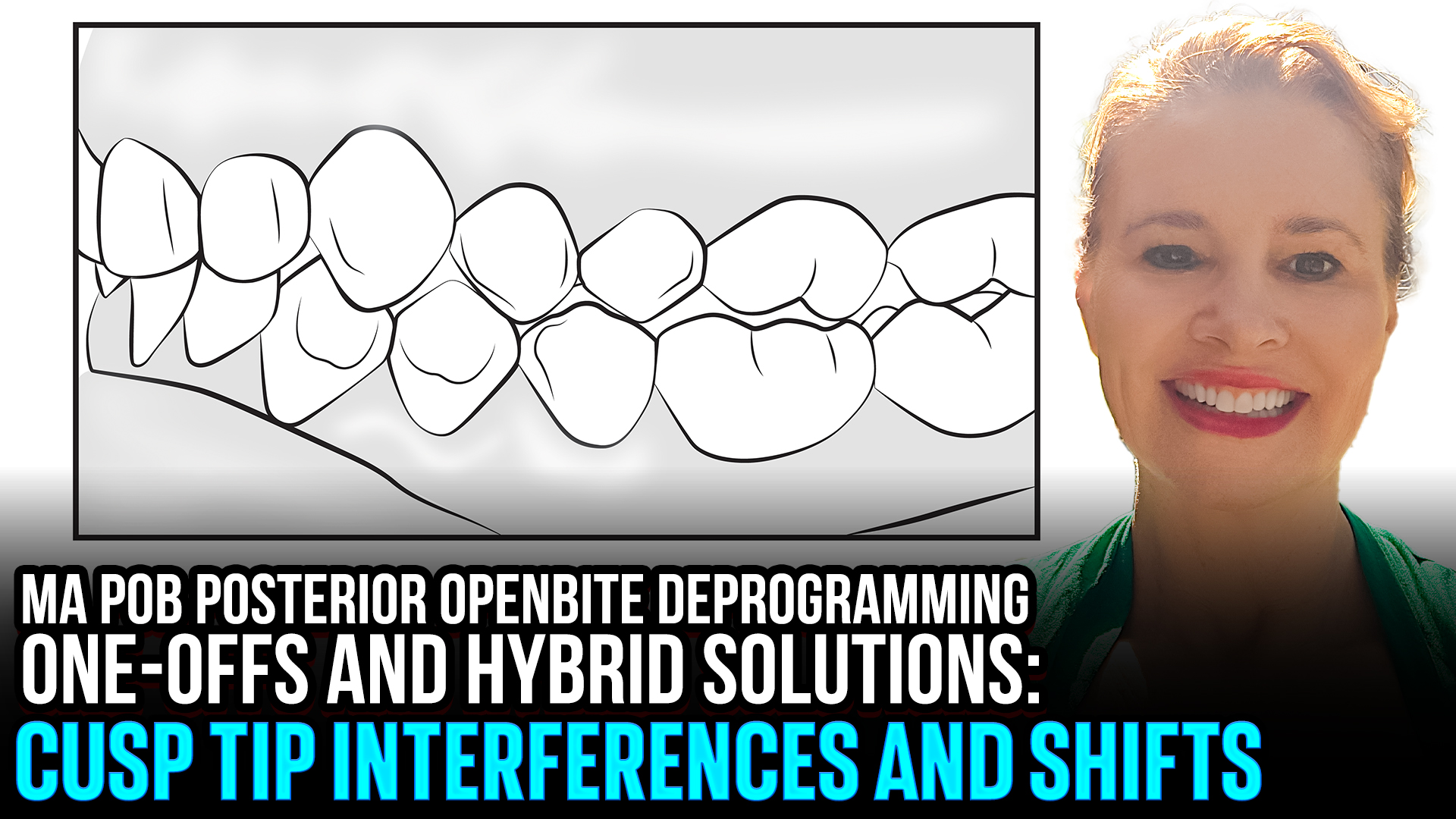
Advanced Hybrid Invisalign with MA: Managing Posterior Open Bite (POB) and Cusp Deprogramming
 Advanced Hybrid Invisalign with MA: Managing Posterior Open Bite (POB) and Cusp Deprogramming
Advanced Hybrid Invisalign with MA: Managing Posterior Open Bite (POB) and Cusp Deprogramming
Introduction
Dr. Amanda discusses a common but often misunderstood challenge following Invisalign with Mandibular Advancement (MA): posterior open bites (POBs) that fail to settle. These cases are frequently misattributed to incomplete MA settling, when in reality the root cause is often under-expansion of the maxillary arch combined with cusp tip interference. Understanding the biomechanics behind these situations is critical to resolving them efficiently and predictably.
Clinical Drivers of POB After Invisalign with MA
Under-Expansion of the Maxillary Arch
Inadequate transverse development leads to cusp tip collisions
Distobuccal cusp interference (e.g., UL6 / #14) blocks posterior settling
Even minor rotations can prevent full occlusal engagement
Cusp Tip Interference, Not MA Failure
Bite will not settle on its own if cusps are impinging
Waiting longer in MA will not resolve mechanical interference
Requires active orthodontic correction, not time
Lower Arch Management Options
If lower teeth are well aligned:
Consider a sloppy bonded appliance to allow natural settling
If lower teeth remain misaligned:
Use a mini-aligner setup (4–4 or 5–5 depending on contacts)
Emphasize extra retention to support passive eruption
Allow settling rather than forcing extrusion
Upper Arch Strategy
Continue maxillary expansion to eliminate transverse discrepancy
Maintain alignment and leveling during expansion
Apply an “unraveling” approach to remove cusp interferences gradually
Foundational Orthodontic Principles
These are basic orthodontic mechanics, not aligner software solutions
Invisalign alone does not teach the diagnosis of occlusal interference
Phase 1 orthodontics and straight-wire fundamentals are essential
Conclusion
Posterior open bites following Invisalign with MA are rarely a timing issue and almost always a biomechanical one. Without addressing maxillary width, cusp interference, and proper deprogramming strategies, these cases will stall indefinitely. Dr. Amanda emphasizes that mastering foundational orthodontics is essential before attempting advanced aligner workflows for predictable and stable outcomes.
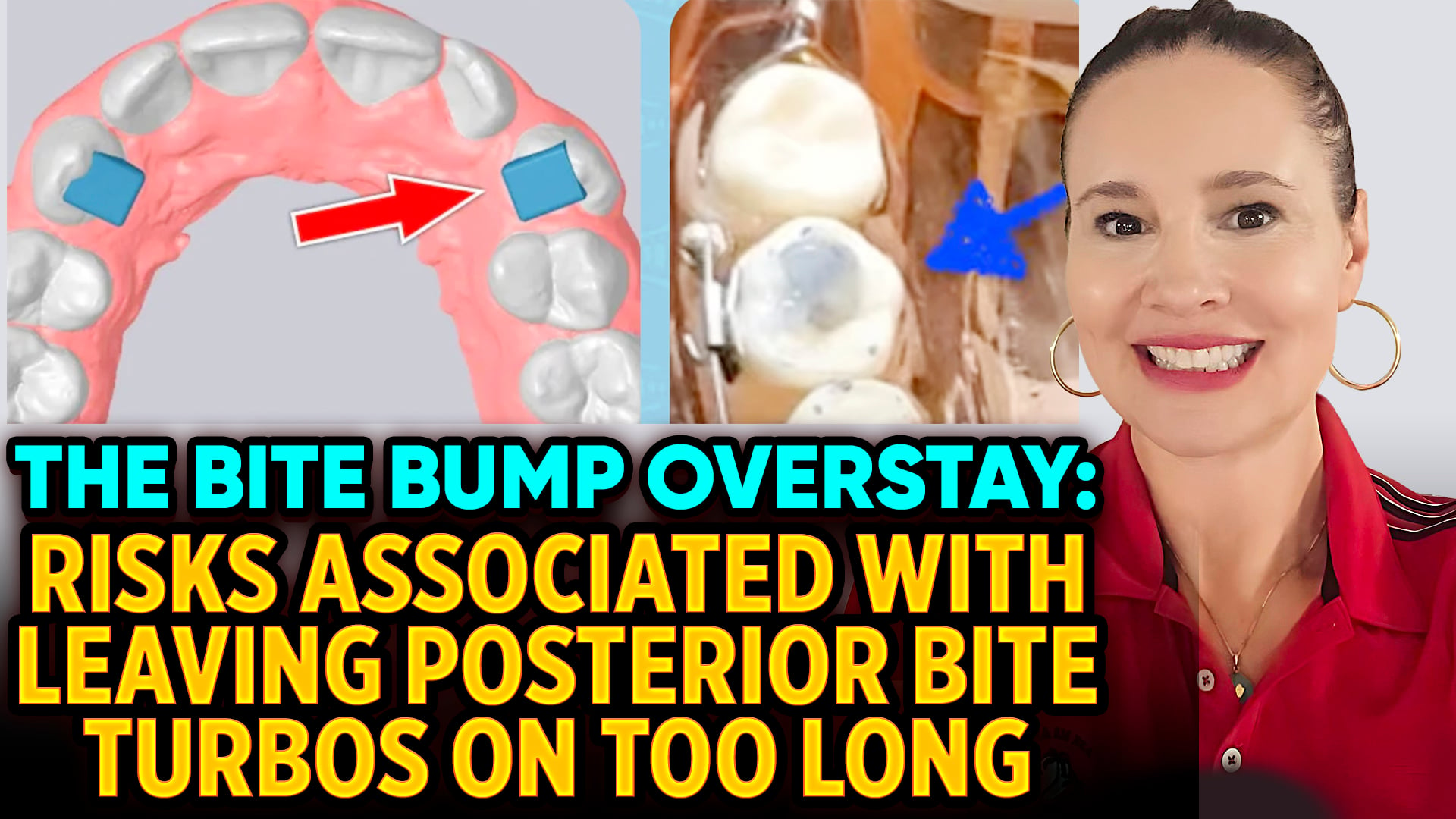
Posterior Bite Bumps
Posterior Bite Bumps (Turbos): Dangerous or Just Bad Orthodontics? How to Manage Risks Safely Through Proper Case Selection
Introduction
Dr. Amanda of Straight Smile Solutions discusses posterior bite turbos, also known as bite bumps or bite ramps, and explains why they pose significant biological and medicolegal risks when used improperly. While bite turbos can be effective for opening the bite in braces cases, she emphasizes that they should be used rarely as part of routine treatment. Poor planning, incorrect placement, and prolonged use can turn a short-term aid into a long-term liability.
Clinical Risks and Management Considerations
What Posterior Bite Bumps Do
- Composite placed on posterior teeth to temporarily open the bite
- Commonly used in braces cases to prevent bracket interference
- Forces are concentrated on individual teeth (unlike aligners, where forces are distributed)
Why They Can Be Dangerous
- Excessive force loading on a single tooth
- Increased risk of:
- Root resorption
- PDL trauma
- Tooth mobility or damage
- Patient discomfort and pain
- Using only one bite bump is especially harmful and should be avoided
Common Clinical Mistakes
- Leaving bite turbos on for months or years
- Forgetting they are present
- Poor tooth selection or excessive height
- Using them routinely instead of proper treatment planning
Risk Management Requirements
- Bite turbos should never be part of a default plan
- Must be monitored at least every 4 weeks
- Chart alerts and removal deadlines are mandatory
- Missed appointments require immediate follow-up
- If used longer than 2–3 months, forces must be distributed across multiple teeth
Preferred Alternatives
- Removable posterior appliances (Gelb/GEL appliances)
- Safer, healthier force distribution
- Best for temporary bite opening when lower teeth interfere with upper movement
- Bite turbos are only justified when patients refuse removable options
Conclusion
Posterior bite turbos are not inherently evil, but careless use is. Dr. Amanda stresses that excellent treatment planning should make them rare, short-term, and closely supervised. When used thoughtfully, documented carefully, and removed promptly, risks are minimized. When overused or forgotten, they represent poor mechanics and unnecessary danger.
I Am SO Excited to Show You the ORIGINAL Keyless RPE / RME Expander Demo Video.

Introduction
Dr. Amanda from Straight Smile Solutions shares her excitement after traveling to Boston to meet the team behind the original keyless RPE/RME expander, developed by Aegis Star in collaboration with the Kellis family. This innovation predates many newer keyless expanders and offers a practical, patient-friendly alternative to traditional key-activated appliances, without the need for excessive lab fees, certifications, or corporate gatekeeping.
Why a Keyless Expander?
What It Is
- A true keyless RPE/RME expander
- Activates without a separate key
- Available in banded or 3D-printed formats
- Performs all functions of a traditional Hyrax
How It Activates
- Simple finger activation
- Each activation delivers 0.2 mm of expansion
- Pull down to activate return to neutral
- No back-spiraling or loss of activation
Why This Matters Clinically
- Eliminates common issues with keys:
- Lost keys
- Difficulty seeing the keyhole
- Poor caregiver compliance
- Visual or dexterity limitations (parents, grandparents)
- Improves overall patient and family experience
Cost and Accessibility
- Only slightly more expensive than a traditional Hyrax
- No required certifications
- No $700–$800 lab fees
- Designed as an option, not a replacement for all cases
Philosophy Behind the Product
- Developed by a family-owned company
- Not venture-capital driven
- Focused on ethical, patient-centered interceptive orthodontics
- Ideal for thoughtful case selection and experienced providers
Conclusion
The original keyless expander offers a simple yet powerful upgrade for the right patient and the right doctor. It’s not about abandoning traditional expanders; it’s about having better options. For clinicians seeking improved compliance, fewer activation issues, and a smoother patient experience without corporate strings attached, this innovation is worth considering. More educational content and demos are coming soon from Dr. Amanda and the Kellis team.
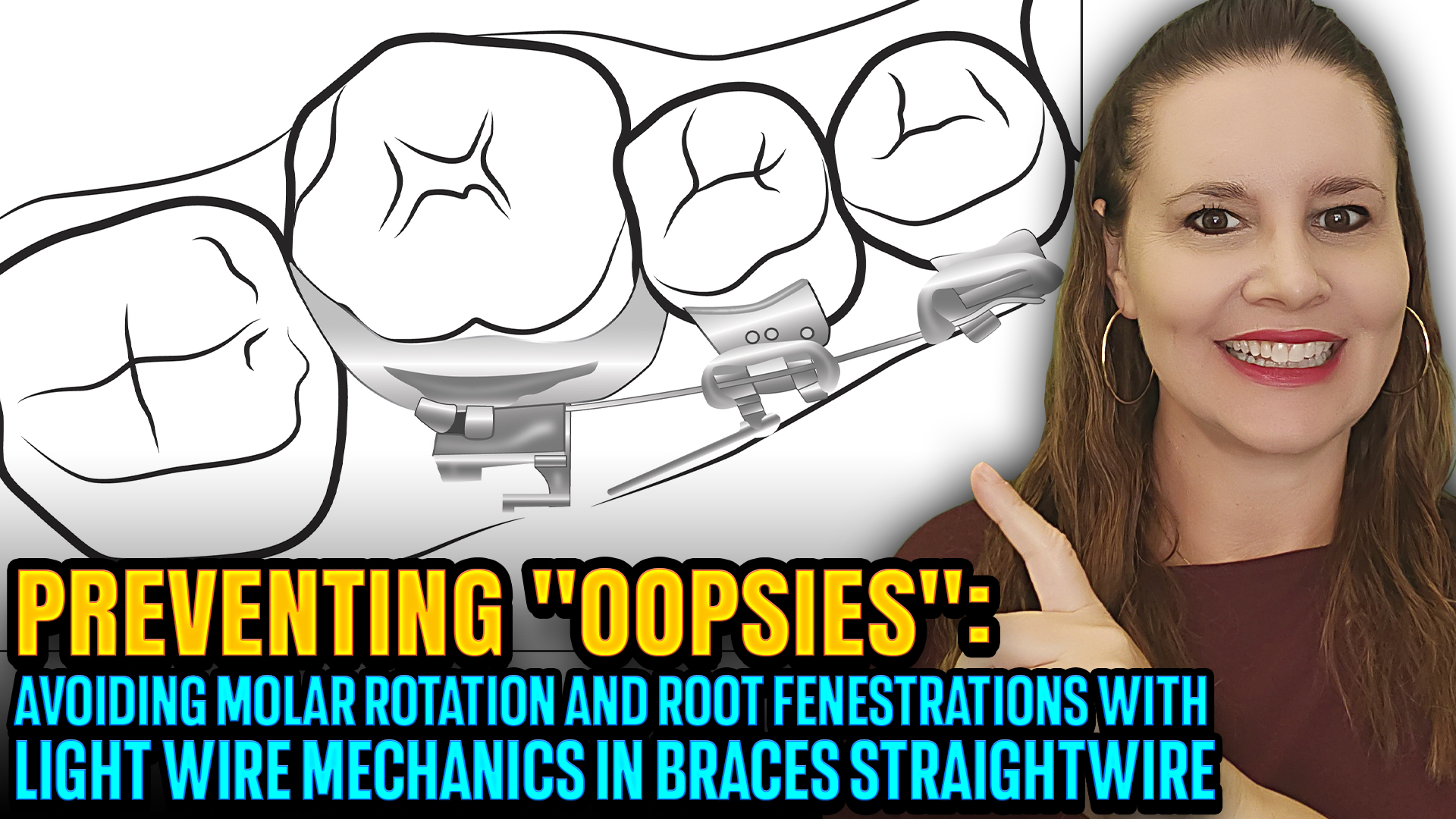
Avoiding Straightwire / Lightwire “OOPSIES”: Tooth Rotation and Fenestrations from Short Wires
Introduction
Dr. Amanda from Straight Smile Solutions highlights a commonly overlooked but serious braces complication: unintended tooth rotation and even fenestration caused by improperly sized straight or light archwires. These “oopsies” are not advanced biomechanics failures; they are preventable setup and monitoring errors that can carry real clinical and legal consequences if missed.
How Short Wires Create Problems
How Straightwire Mechanics Are Designed to Work
- Archwires are meant to fully engage brackets and extend slightly past the molar tubes
- A small amount of wire exiting the tube ensures:
- Full force expression
- Balanced push–pull mechanics
- Proper counter-moments to control rotation
What Goes Wrong with Short Wires
-
- Over-trimming the wire during placement
- Only the tip of the wire engages the molar tube
- The remainder of the tube span is empty
- Results in:
- Force applied in only one direction
- Loss of counterforce
- Progressive, unintended tooth rotation
Why This Can Become Dangerous
-
- Continued unbalanced force can push a tooth outside the alveolar bone
- Risk of:
- Fenestration
- Dehiscence
- Bone loss
- Liability for the treating doctor
- Often missed when patients disappear for weeks or months
Not Always a Staff Error
- Light wires can shift over time
- Common in:
- Long spans
- Mixed dentition
- Areas near unerupted teeth
- A shifted wire may partially disengage from the tube without anyone noticing
Prevention Strategies
- Always confirm the wire fully passes through the molar tubes
- Ensure visible wire extension before trimming
- Monitor light wires closely at every visit
- Consider cinching only when biomechanically appropriate
- Never assume “it’s in the tube” without visual confirmation
Conclusion
These straightwire “oopsies” are preventable with attention to detail and consistent monitoring. Even simple mechanics can cause serious damage if a wire disengages unnoticed. Dr. Amanda’s core message: If you’re wearing braces, you must anticipate emergencies, monitor them actively, and never rely on assumptions.
Is Your Invisalign Aligner Really Off Track? Refinement Alternatives—Backtracking and Chewies

Introduction
Dr. Amanda of Straight Smile Solutions addresses one of the most common clinical questions in clear aligner therapy: how to determine whether an Invisalign aligner is truly off track. She explains that not every visible gap is a treatment failure and that most tracking issues can be prevented or corrected without immediately moving to refinement. Proper patient education, correct use of aligners, saving old aligners, and a careful review of the Tooth Movement Table (TMT) are essential for making informed clinical decisions.
Key Clinical Considerations
Chewies and Patient Compliance
- Chewies are often given without proper instruction, limiting their effectiveness
- Ortho Munchies offer a more intuitive design with grooves for different tooth groups
- Instructional videos help patients perform chewing exercises correctly and consistently
- Creating a practice-specific chewy protocol can improve compliance and differentiate the practice
Evaluating True Tracking Issues
- Always review the Tooth Movement Table (TMT) before assuming loss of tracking
- Each aligner may be programmed for intrusion, extrusion, rotation, torque, or root movement
- Some movements, especially intrusion, can appear off track due to thicker plastic
- Visual gaps must be interpreted in the context of the planned movement
Clinical Response Based on Severity
- Small gaps: acceptable; reinforce chewy use and monitor
- Moderate gaps: hold the patient in the same aligner or backtrack
- Large gaps: indicate true loss of tracking and require refinement
Backtracking as a First-Line Solution
- Patients should always save and bring old aligners to appointments
- Backtracking one or two trays is often faster than refining
- Extended wear may discolor aligners, making replacement trays necessary
Monitoring and Workflow
- Virtual monitoring allows early detection of tracking issues
- Consistent review makes identifying problems faster and more predictable
Conclusion
Not every aligner discrepancy represents a true tracking failure. By analyzing programmed movements, educating patients on the proper use of chewy products, utilizing backtracking when possible, and closely monitoring progress, clinicians can resolve most Invisalign tracking issues efficiently, avoiding unnecessary refinements and saving valuable chair time.
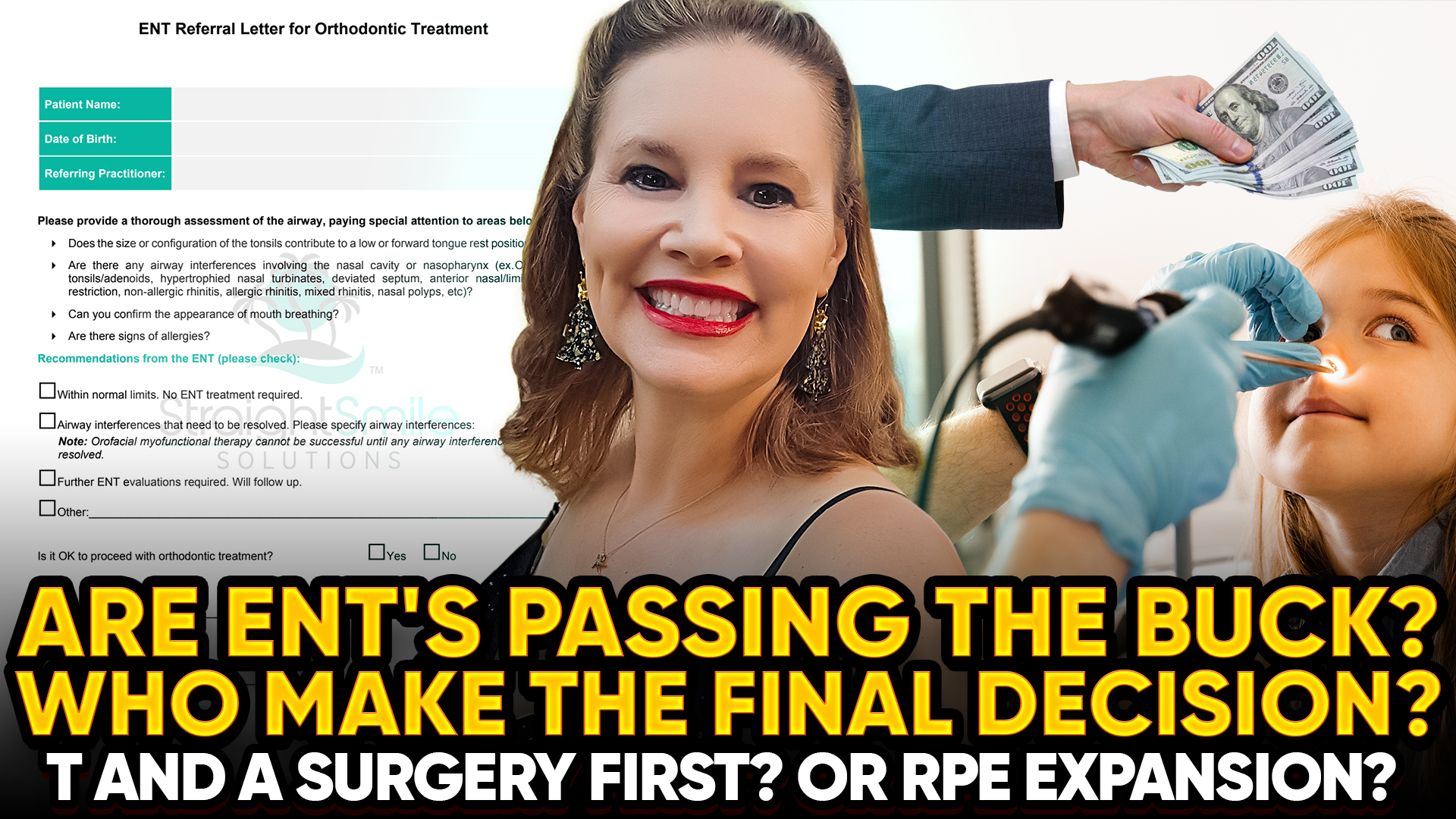
Working with ENTs on Airway and Expansion Cases: Are They Passing the Buck? The Importance of Documentation
Introduction
Dr. Amanda addresses a critical and increasingly common challenge in early orthodontic and Phase I cases: managing potential airway concerns while collaborating appropriately with ENT physicians. As awareness around airway health grows, orthodontists and dentists must balance orthodontic treatment, medical responsibility, and legal risk. Clear communication, proper referrals, and thorough documentation are essential, not optional.
Key Considerations When Collaborating with ENTs
Orthodontics vs. Medical Responsibility
• Orthodontists treat orthodontic problems, not medical airway conditions
• Suspected airway pathology requires physician (ENT) involvement
• Orthodontic treatment may incidentally improve the airway, but this cannot be promised
When to Delay Orthodontic Treatment
• Do not start expansion if a severe airway issue is suspected
• Fixed appliances can temporarily worsen the airway by reducing oral volume
• ENT diagnostics and treatment planning should come first
Hierarchy of Care
• ENTs determine medical and surgical necessity
• Medical and surgical decisions take precedence over orthodontics
• Orthodontic treatment may proceed only after ENT clearance
Get Everything in Writing
• Never rely on the patient’s verbal report
• Use a written ENT communication form or referral letter
• If the ENT defers or declines intervention, document that decision
Documentation Protects You
• Written confirmation reduces liability and risk exposure
• Document orthodontic indications separately and clearly
• Monitor orthodontic progress while the ENT monitors airway health
Removable Appliances and Airway Awareness
• Removable expanders (e.g., IP) may be safer during evaluation
• Inability to tolerate appliances, especially at night, may signal airway issues
• Do not force compliance when red flags appear
Professional Collaboration Matters
• Bulldozing ENTs damages trust and professional credibility
• Build referral relationships through education and communication
• Younger ENTs may be more open to collaboration and current research
Conclusion
Managing airway adjacent orthodontic cases requires humility, teamwork, and meticulous documentation. Dr. Amanda emphasizes that ethical care means collaborating, not competing with ENTs, respecting the medical hierarchy, and protecting patients through clear and accurate records. When in doubt: document, communicate, and prioritize patient safety above all else.