I. Introduction
Dr. Amanda from Straight Smile Solutions explains a structured approach to evaluating airway health in Phase 1 interceptive orthodontic patients.
The focus is on proper screening before orthodontic treatment, especially in children.
She emphasizes that jumping straight into orthodontics without airway evaluation can worsen outcomes.
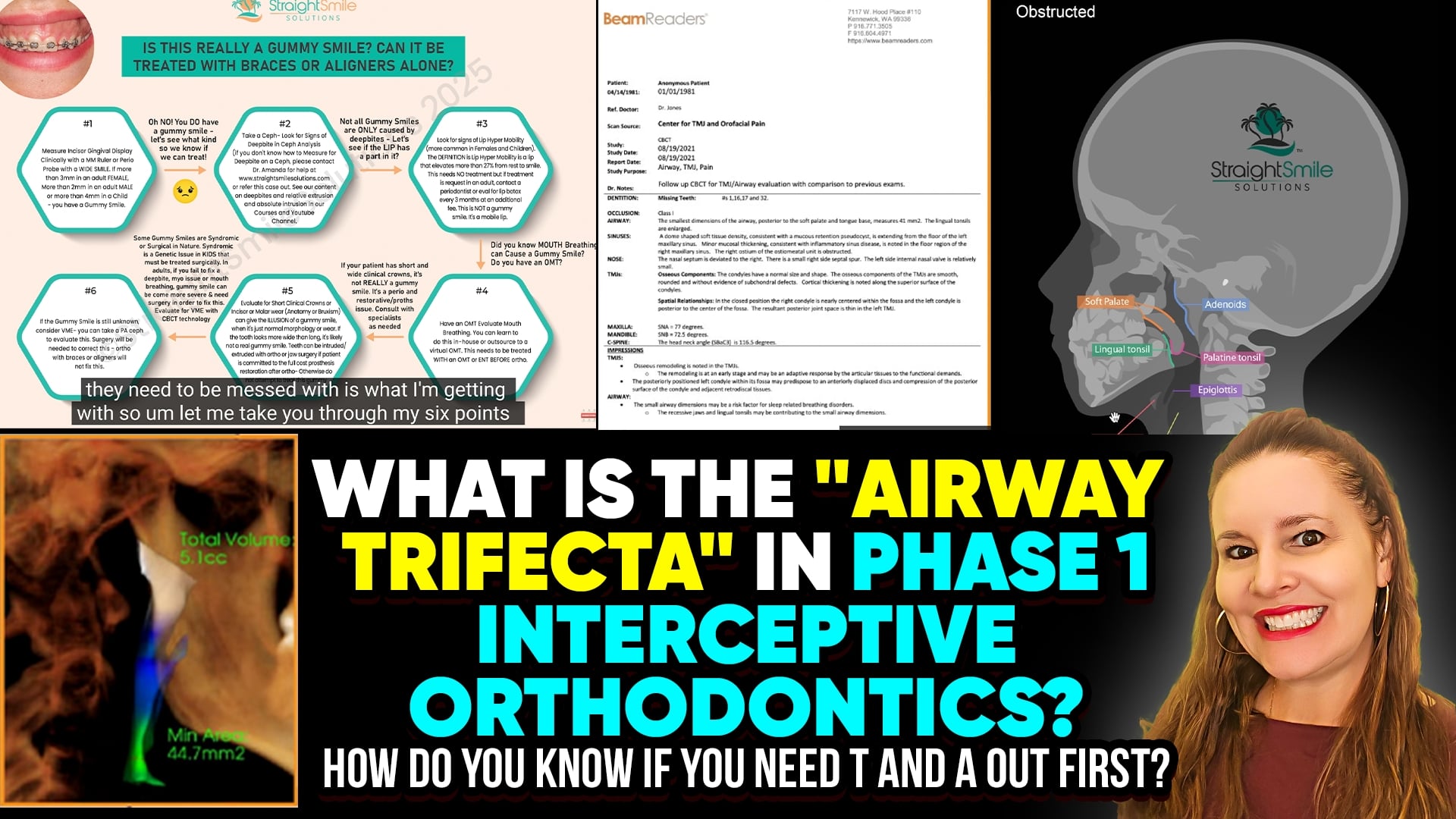
The concept of the “Airway Trifecta” highlights the most critical red flags that must be assessed first.
II. Airway Trifecta and Comprehensive Screening
Subjective Screening
Use structured questionnaires completed at home, not in the office.
Parents should observe the child’s sleep over multiple nights.
Video recordings of breathing or sleep disturbances are strongly encouraged.
Watch for snoring, mouth breathing, restless sleep, and pauses in breathing.
Daytime Behavioral and Physical Red Flags
Chronic mouth breathing observed in the waiting room.
Daytime sleepiness or fatigue.
ADHD-like behaviors and poor focus (correlation, not causation).
Nocturnal enuresis (bedwetting).
Dark circles under the eyes.
“Airway face” characteristics.
Objective Clinical Screening
Long facial growth patterns.
Narrow arches and vertically excessive growth.
Gummy smiles linked to airway dysfunction.
Small or constricted airways seen on lateral ceph or CBCT.
Radiology reports suggesting potential airway compromise.
Myofunctional (Myio) Screening
In-office screening by the orthodontist is essential.
Identification of tongue posture issues, swallowing dysfunction, and oral habits.
Referral to a myofunctional therapist when multiple red flags are present.
Recognition that myofunctional therapy is time-intensive and specialized.
Interdisciplinary Referrals
ENT evaluation when tonsils, adenoids, or nasal obstruction are suspected.
Myofunctional therapy before orthodontics when habits persist.
Avoid initiating orthodontics until airway, habits, and obstruction are addressed.
Treatment Planning Across All Planes of Space
Expansion alone is often insufficient.
Consider sagittal (AP), vertical, and transverse discrepancies.
Jaw positioning and bite correction may be required.
Untreated airway or habit issues increase relapse risk.
III. Conclusion
The “Airway Trifecta” reinforces the importance of thorough subjective and objective screening, myofunctional evaluation, and interdisciplinary collaboration before Phase 1 orthodontic treatment. Addressing airway health first protects both the patient and provider, reduces relapse, and leads to more stable, functional outcomes. Knowing when to delay treatment and refer is a sign of responsible, airway-centered orthodontic care.