StraightSmile Solutions®
Is Invisalign’s “Pay Per Aligner” Program Worth It?
 Is Invisalign’s “Pay Per Aligner” Program Worth It?
Is Invisalign’s “Pay Per Aligner” Program Worth It?
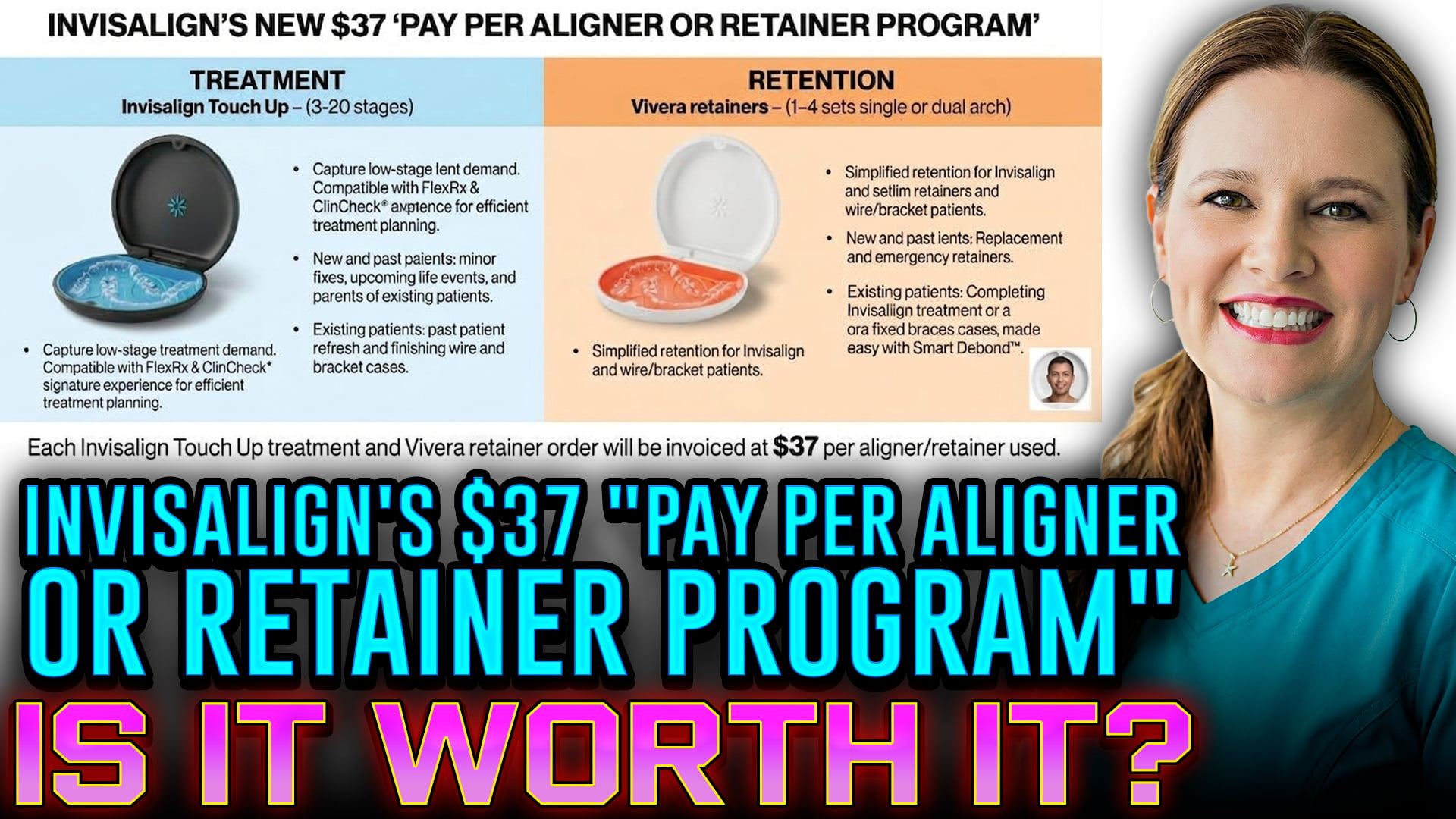
A new feature on the Invisalign dashboard has dental professionals talking. Invisalign is introducing a “Pay Per Aligner or Retainer” program. This shift aims to offer doctors and patients more flexibility with clear aligner treatment pricing. However, it also introduces unique challenges for modern dental practices.An Opportunity for Patients and DoctorsThis pay-per-aligner model can be incredibly beneficial. For patients, it provides a highly customizable entry point into orthodontic treatment. Individuals who only need minor touch-ups or specific standalone retainers no longer have to commit to expensive comprehensive packages. Doctors can utilize this program to offer targeted, cost-effective adjustments. It can also build a robust aftercare program for long-term retention.The Industry ShiftDespite the convenience, this model represents what many in the industry call a “race to the bottom”. Decades ago, clear aligner orthodontics was a premium, high-margin service. Today, the market is highly commoditized. Once patients discover the base lab fees for individual aligners, practices may face heavy pressure to lower their consumer pricing. This shift can make it incredibly difficult to maintain standard profit margins on basic treatments.Strategic Solutions for Your PracticeTo survive this changing landscape, general and pediatric dentists must adapt their business strategies. Relying solely on standard adult aligner cases is no longer a viable long-term strategy for high profitability. Instead, practices should focus on complex phase-one interceptive treatments and growth modifications. Additionally, dentists must learn to properly monetize their aftercare and retention programs. Offering structured long-term maintenance packages ensures stable revenue while protecting patient smiles.If you are a dental professional navigating these new pricing structures, consider evaluating your current overhead. I can help you analyze your lab fees, design an aftercare subscription, or explore phase-one tracking strategies.
How Smartee’s Technology is Transforming Straumann’s ClearCorrect
Navigating the DSO Landscape: How to Protect Your Dental Career
ClearCorrect vs. Invisalign: CBCT Functionality Compared

Rethinking Phase Orthodontics: Do Your Patients Really Need It?

Why You Need an Orthodontic and Airway Evaluation Before Plastic Surgery
 Why You Need an Orthodontic and Airway Evaluation Before Plastic Surgery
Why You Need an Orthodontic and Airway Evaluation Before Plastic Surgery
Are you considering a rhinoplasty or a chin advancement to enhance your facial profile? Before you book that consultation with a plastic surgeon, there is a critical step you might be missing. Seeking an orthodontic and airway evaluation first can completely change your treatment outcome—and potentially save you thousands of dollars.The Hidden Link Between Structure and BreathingYour nose, jaw, and teeth do not exist in isolation. They form a complex, interconnected system that dictates how you look, bite, and breathe. Often, what appears to be a purely cosmetic concern is actually a sign of an underlying structural issue. For instance, a crooked or deviated nose resulting from a childhood injury isn’t just an aesthetic flaw; it frequently causes significant airway compromise, making it harder to breathe properly through your nose.Why Orthodontics Comes FirstEvaluating your bite and jaw alignment before undergoing plastic surgery ensures that any cosmetic changes do not accidentally worsen your breathing or oral health. An orthodontist can look at the big picture. If your chin appears recessed, the root cause might be a misaligned jaw that requires structural correction rather than a simple cosmetic implant. Addressing the foundation first ensures your aesthetic results look natural and last a lifetime.The Insurance AdvantageHere is the most compelling reason to start with a medical evaluation: financial coverage. If an airway assessment proves that your breathing is compromised due to structural trauma, your procedure moves from “cosmetic” to “medically necessary.” In many instances, health insurance will cover a rhinoplasty or reconstructive surgery if it corrects a functional deficit.
Flying Safely: Can You Board a Plane with a Toothache?
 Flying Safely: Can You Board a Plane with a Toothache?Taking to the skies with a sudden toothache can turn a dream vacation into a painful nightmare. The unique environment inside an airplane cabin has a surprising impact on dental health. Understanding how cabin pressure affects your teeth is essential for a safe and comfortable journey.The primary culprit behind mid-flight dental pain is a phenomenon called barodontalgia, commonly known as “tooth squeeze.” As an airplane climbs, atmospheric pressure drops, causing pockets of trapped air to expand. If you have an untreated cavity, a cracked filling, or a hidden infection at the root of a tooth, the air trapped inside those microscopic spaces expands rapidly. This internal pressure pushes directly against the sensitive nerves of your teeth, causing sudden, sharp, and sometimes excruciating pain.While a mild ache might feel manageable on the ground, the pressure shift during a flight can amplify the discomfort dramatically. More importantly, flying with an active dental infection or an abscess carries serious risks. The changing pressure can alter blood flow and potentially worsen the inflammation or spread the infection, which can lead to severe medical complications mid-flight.To protect your health, scheduling a dental checkup before any long-haul flight is a smart strategy. Dentists can identify hidden issues and ensure your fillings are secure. If you absolutely must fly with a minor toothache, pack over-the-counter pain relievers and a cold compress in your carry-on luggage. Staying hydrated and avoiding extremely hot or cold beverages during the flight will also help minimize nerve irritation.Prioritizing your dental health ensures a smooth journey. Never ignore dental pain before boarding. A quick visit to a professional can save your trip and keep your smile intact.Would you like some tips on how to handle a dental emergency while traveling abroad?1
Flying Safely: Can You Board a Plane with a Toothache?Taking to the skies with a sudden toothache can turn a dream vacation into a painful nightmare. The unique environment inside an airplane cabin has a surprising impact on dental health. Understanding how cabin pressure affects your teeth is essential for a safe and comfortable journey.The primary culprit behind mid-flight dental pain is a phenomenon called barodontalgia, commonly known as “tooth squeeze.” As an airplane climbs, atmospheric pressure drops, causing pockets of trapped air to expand. If you have an untreated cavity, a cracked filling, or a hidden infection at the root of a tooth, the air trapped inside those microscopic spaces expands rapidly. This internal pressure pushes directly against the sensitive nerves of your teeth, causing sudden, sharp, and sometimes excruciating pain.While a mild ache might feel manageable on the ground, the pressure shift during a flight can amplify the discomfort dramatically. More importantly, flying with an active dental infection or an abscess carries serious risks. The changing pressure can alter blood flow and potentially worsen the inflammation or spread the infection, which can lead to severe medical complications mid-flight.To protect your health, scheduling a dental checkup before any long-haul flight is a smart strategy. Dentists can identify hidden issues and ensure your fillings are secure. If you absolutely must fly with a minor toothache, pack over-the-counter pain relievers and a cold compress in your carry-on luggage. Staying hydrated and avoiding extremely hot or cold beverages during the flight will also help minimize nerve irritation.Prioritizing your dental health ensures a smooth journey. Never ignore dental pain before boarding. A quick visit to a professional can save your trip and keep your smile intact.Would you like some tips on how to handle a dental emergency while traveling abroad?1
Beyond Western Medicine: Holistic Relief for Jaw Pain and Bruxism
 Beyond Western Medicine: Holistic Relief for Jaw Pain and BruxismSevere jaw clenching and TMJ pain can severely impact your quality of life. Traditional Western medicine often treats bruxism with skeletal muscle relaxers like cyclobenzaprine. While highly effective for temporary relief, these controlled substances are unsafe for long-term nightly use. Other mainstream options like Botox are incredibly expensive and carry potential long-term side effects. When standard dental treatments fail to halt severe chronic pain, turning to holistic, non-pharmaceutical alternatives can provide a transformative breakthrough.The underlying cause of severe jaw tension is often deeply connected to the nervous system. For instance, individuals experiencing high stress, neurodivergence, or hormonal transitions like perimenopause can suffer from sudden, endogenous cortisol storms. This systemic surge of adrenaline and cortisol causes the neuroendocrine system to become highly volatile, directly forcing the jaw mechanics to lock up in an intensely painful state. When standard anti-inflammatory medications are no longer an option due to the risk of kidney strain, a holistic approach becomes necessary to address the root stress response.Sound therapy and targeted physical manipulation offer a powerful, natural path to resetting a locked jaw. Sound vibration sessions using therapeutic bowls and gongs create deep auditory waves that encompass the body, prompting immediate, involuntary muscle relaxation. To maintain this relief, practicing myofascial release using simple tools like yoga blocks and tennis balls can successfully target and break down stubborn tension in the jaw and neck muscles. Shifting away from heavy pharmaceuticals allows you to work in harmony with your biology. Embracing alternative therapies can restore your physical comfort and provide lasting, holistic healing.
Beyond Western Medicine: Holistic Relief for Jaw Pain and BruxismSevere jaw clenching and TMJ pain can severely impact your quality of life. Traditional Western medicine often treats bruxism with skeletal muscle relaxers like cyclobenzaprine. While highly effective for temporary relief, these controlled substances are unsafe for long-term nightly use. Other mainstream options like Botox are incredibly expensive and carry potential long-term side effects. When standard dental treatments fail to halt severe chronic pain, turning to holistic, non-pharmaceutical alternatives can provide a transformative breakthrough.The underlying cause of severe jaw tension is often deeply connected to the nervous system. For instance, individuals experiencing high stress, neurodivergence, or hormonal transitions like perimenopause can suffer from sudden, endogenous cortisol storms. This systemic surge of adrenaline and cortisol causes the neuroendocrine system to become highly volatile, directly forcing the jaw mechanics to lock up in an intensely painful state. When standard anti-inflammatory medications are no longer an option due to the risk of kidney strain, a holistic approach becomes necessary to address the root stress response.Sound therapy and targeted physical manipulation offer a powerful, natural path to resetting a locked jaw. Sound vibration sessions using therapeutic bowls and gongs create deep auditory waves that encompass the body, prompting immediate, involuntary muscle relaxation. To maintain this relief, practicing myofascial release using simple tools like yoga blocks and tennis balls can successfully target and break down stubborn tension in the jaw and neck muscles. Shifting away from heavy pharmaceuticals allows you to work in harmony with your biology. Embracing alternative therapies can restore your physical comfort and provide lasting, holistic healing.
Navigating White-Label Aligner Brands: Clinical Consulting vs. Digital Tech Setup
- Staging biomechanics and predictability
- Transverse expansion limits
- Interproximal reduction (IPR) timing and placement
- Anchorage requirements, such as elastics or specialized attachments

Accessing Free Orthodontic Documents, Consent Forms, and Support for Your Dental Practice