StraightSmile Solutions®
Navigating White-Label Aligner Brands: Clinical Consulting vs. Digital Tech Setup
- Staging biomechanics and predictability
- Transverse expansion limits
- Interproximal reduction (IPR) timing and placement
- Anchorage requirements, such as elastics or specialized attachments

Accessing Free Orthodontic Documents, Consent Forms, and Support for Your Dental Practice
Mastering ClearCorrect Aligners: A Comprehensive Guide to Mandibular Advancement Repositioning
 Mastering ClearCorrect Aligners: A Comprehensive Guide to Mandibular Advancement Repositioning
Mastering ClearCorrect Aligners: A Comprehensive Guide to Mandibular Advancement Repositioning
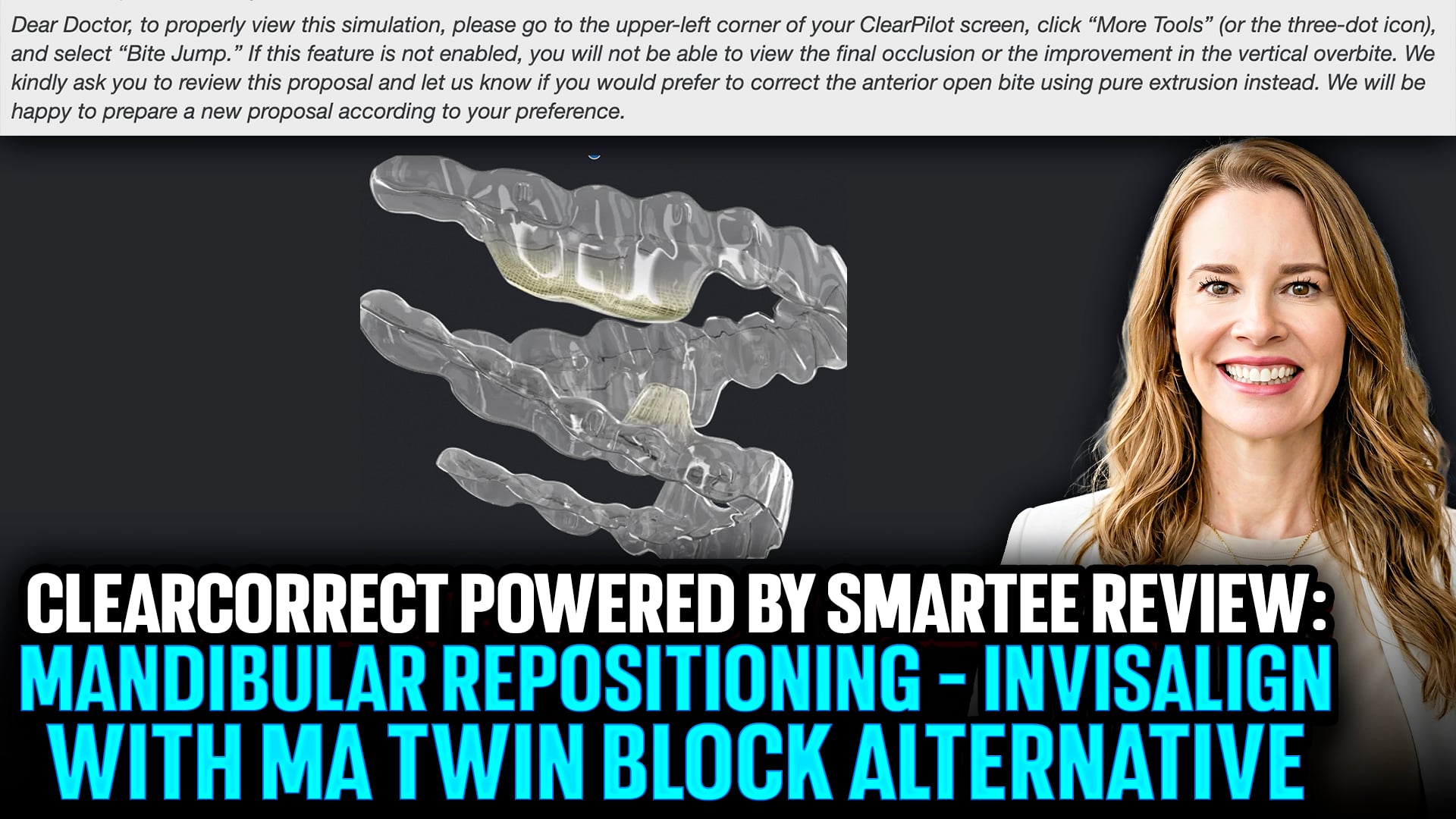
The clear aligner landscape is constantly shifting as companies look for ways to break into new therapeutic territories. For years, Invisalign held a firm grip on the clear aligner mandibular advancement market. However, a new alternative has officially entered the ring: ClearCorrect MA, powered by Smartee. This feature, referred to as mandibular repositioning (MR), offers general and pediatric dentists a fresh option for treating Class II malocclusions.First Impressions and DesignAt first glance, the ClearCorrect MR feature looks like a hybrid between traditional wings and blocks. Because the technology utilizes a slightly different form than existing options, it avoids intellectual property issues while remaining FDA approved. At its core, the appliance operates on standard biomechanics—it functions as a clear aligner equipped with a ski ramp to prompt forward mandibular posture.Current Software LimitationsWhile the underlying clinical mechanics are promising, the digital integration leaves room for improvement. The current iteration of the ClearPilot dashboard struggles to accurately visualize the full bite jump. Unlike more mature platforms that seamlessly demonstrate incremental movements and account for functional shifts, ClearCorrect’s current graphics can feel unpolished. This disparity likely stems from integration hurdles between Smartee’s native platform and ClearCorrect’s software interface. Furthermore, communication with digital lab technicians requires precision, as they may not intuitively recognize complex skeletal shifts yet.Clinical ImplementationTransitioning a patient out of these appliances is not a direct path. Practitioners cannot simply jump from a mandibular repositioning aligner straight into standard finishing clear aligners without an intermediate step. Implementing a strict deprogramming protocol is essential to ensure the jaw stabilizes correctly before finalizing the treatment plan. Though the software feels like an early-stage release, this tool expands the orthodontic toolkit for providers comfortable managing the clinical nuances.
Custom vs. Traditional Orthognathic Jaw Surgery: A Guide for Dental Professionals
 Custom vs. Traditional Orthognathic Jaw Surgery: A Guide for Dental ProfessionalsT
Custom vs. Traditional Orthognathic Jaw Surgery: A Guide for Dental ProfessionalsT
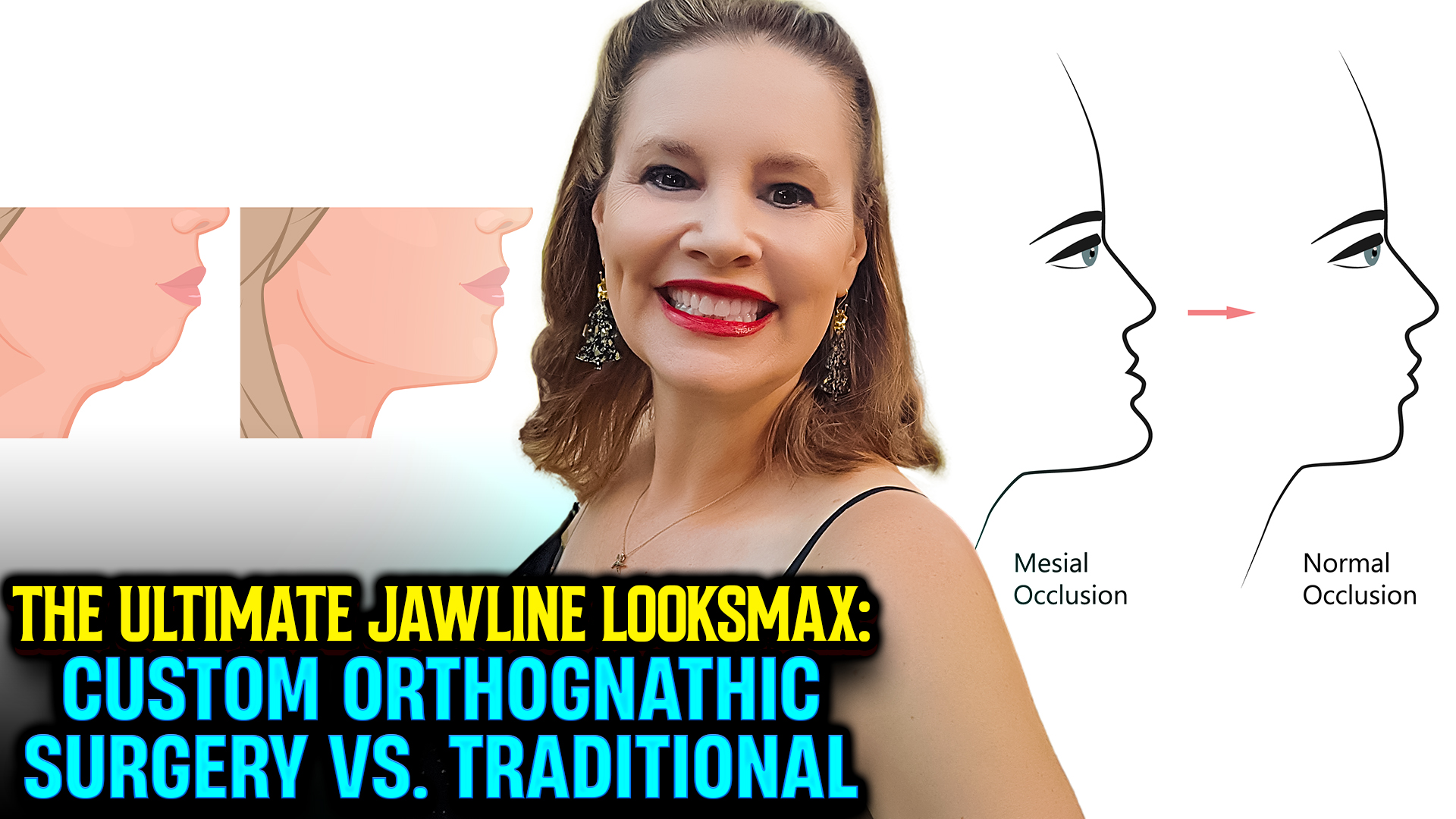
he dental industry is experiencing a massive paradigm shift. Between shifting clinical perspectives on Reddit, public blogs, and the explosion of myofunctional therapy (OMT), patients and practitioners alike are looking more closely at how we correct severe jaw discrepancies. The biggest conversation right now surrounds custom orthognathic surgery versus traditional orthognathic surgery.Traditional orthognathic surgery relies on standard diagnostic models, digital tracings, and stock cephalometric norms. Patients generally undergo two to three years of decompensation using traditional braces or Invisalign before they are ready for the operating room. During the procedure, the oral surgeon uses stock titanium plates, which must be manually bent during surgery to fit the patient’s anatomy. Treating strictly to “cephalometric norms” can leave some patients with flat-looking facial aesthetics, and the multi-year timeline frequently causes severe patient burnout.Custom orthognathic surgery shifts the focus from rigid mathematical norms to a completely face-focused setup. Because the movements are mapped out ahead of time with immense digital accuracy, clinicians can often execute the surgery much earlier in the timeline—sometimes before braces or aligners are even placed. This workflow utilizes 100% patient-specific, 3D-printed guides and pre-printed metal or plastic plates. The surgeon skips the guesswork of bending plates mid-operation. This level of customization delivers drastically superior cosmetic and structural outcomes.While custom jaw surgery yields incredible outcomes, the financial and administrative structures require careful management from the provider side. Custom surgery takes 5 to 10 times more doctor planning time. While traditional orthodontic fees range from $6,000 to $9,000, custom cases range from $8,000 to $12,000, plus an additional $3,000 to $4,000 for separate lab hardware fees. Because insurance rarely covers premium 3D-printed hardware, parents face high out-of-pocket costs. Charging a substantial upfront planning fee helps mitigate financial risk and prevents the clinical damage caused by aborted or cancelled surgical cases.
Why “Board Certified” Might Not Mean What You Think in Orthodontics
 Why “Board Certified” Might Not Mean What You Think in Orthodontics
Why “Board Certified” Might Not Mean What You Think in Orthodontics
When choosing an orthodontist, most parents and patients instinctively look for the phrase “Board Certified”. It sounds like the ultimate stamp of clinical excellence. However, the reality behind American Association of Orthodontists (AAO) board certification has drastically changed over the years.
Dr. Amanda from Straight Smile Solutions recently pulled back the curtain on why she—and many other thriving orthodontists—purposely avoid advertising this certification. Here is what you need to know about the shift from rigorous clinical evaluation to digital simulations.The Flawed History of Clinical TestingFor decades, the final step of becoming board-certified required specialists to collect physical stone models and photos of real patients. Doctors had to fly with suitcases full of fragile patient records to a live defense panel.The primary issue with this legacy system was its highly rigid, outdated requirements:Mandatory Extraction Cases: Orthodontists were forced to present cases involving the extraction of four premolars to prove they could manage root parallelism and anchorage control.Ethical Dilemmas: Many modern specialists found these forced extractions ethically problematic, preferring instead to focus on early interceptive care, airway growth, and widening the palate so teeth could fit naturally.Artificial Over-Treatment: Doctors often had to keep patients in braces for extra months simply to polish up a perfect physical model for the testing board.Because of these mandatory standards, many exceptional orthodontists walked away from the process entirely, refusing to prioritize marketing over individualized patient health.The 2019 Pivot to Computer SimulationsIn 2019, the board quietly overhauled the entire certification system, completely abolishing the real-life patient model presentation.Today, an orthodontist can achieve board-certified status without presenting a single real patient case to a live panel. Instead, they sit at a computer monitor in a commercial testing facility and complete a sterile, digital simulation centered strictly around tooth straightening.While this eliminated the ethical issue of forced extractions, critics argue it turned the credential into a corporate marketing gimmick rather than a reflection of true hands-on clinical excellence. Additionally, to maintain the stamp in marketing materials, doctors must continuously pay steep membership dues to the association.Choosing the Right SpecialistA licensed orthodontist has already completed years of rigorous dental school followed by an accredited residency program. Certification is entirely optional.When looking for a provider, focus on their treating philosophy rather than a marketing badge. Many top-tier specialists focus heavily on holistic growth, facial symmetry, and airway health, choosing to let their real-world results speak for themselves.
Navigating Bone Housing with New Aligner Technology
The Vital Role of Early Orthodontic Intervention
 The Vital Role of Early Orthodontic Intervention
The Vital Role of Early Orthodontic Intervention
A major shift is happening in pediatric dentistry toward functional care, focusing on airway health, jaw development, and tongue posture. True early intervention means looking beyond straight teeth to address how a child breathes and functions.Expanding the GarageA helpful analogy compares palatal expansion to widening a garage. Expanding the upper jaw physically lowers the nasal floor, instantly improving airflow and curbing chronic mouth breathing. However, making the garage bigger is only half the battle. If you do not retrain the tongue to rest on the roof of the mouth, the jaw structure will not remain stable.For lasting success, structural expansion must be paired with myofunctional therapy. Dentists need to collaborate with specialized therapists or utilize silicone oral trainers. Retraining the facial and tongue muscles is just as critical as expanding the bone.Rethinking the TimelinesThe standard guideline recommends an orthodontic screening by age seven. However, many general and pediatric dentists wait until a child turns seven to write a referral, meaning the child is often eight before seeing a specialist.True interceptive treatment should start by age seven, meaning referrals must happen at age five or six—before primary teeth even fall out. Waiting until permanent teeth erupt misses the optimal window for skeletal growth guidance and airway development.Fixing the Referral SystemA common issue in traditional orthodontics is holding pediatric cases until age twelve to fix everything in a single, later stage. Unfortunately, ignoring developmental deficits during early childhood harms a child’s systemic health.Primary dentists can change this by sending qualified referrals rather than blank slips. Attaching intraoral scans, sleep studies, and myofunctional data forces specialists to acknowledge immediate functional needs. If local specialists still delay care, general dentists should seek the education necessary to provide this life-changing, early interceptive care themselves.
Unmasking the Friendly Dentist Model: Is Your Local Practice Secretly Corporate?
 Unmasking the Friendly Dentist Model: Is Your Local Practice Secretly Corporate?When you walk into your local dentist or orthodontist’s office, you expect the same familiar faces and the personalized care you have trusted for years. However, behind the scenes, a major shift is occurring across the dental and medical industries. Corporate private equity (PE) firms are quietly buying up independent practices while keeping the original doctor’s name on the building.This strategy is known as the friendly dentist model. It allows corporate entities to take over operations without alerting patients who value local, independent healthcare.Signs your dentist might be secretly corporateBecause private equity firms try to make these transitions invisible, you have to look closely to see if your practice has changed hands.Website footers: Scroll to the absolute bottom of your dentist’s website. Look closely for tiny print using phrases like “powered by,” “affiliated with,” or “partners of” followed by a corporate name.Generic online portals: If the online booking links, digital intake forms, or bill payment portals suddenly look highly generic and unbranded, it might be a standardized corporate platform.High staff turnover: Private equity takeovers often introduce new compensation structures that cause long-term staff to leave. If you notice a steady trickle of new faces at the front desk and in the back office, the culture may have shifted behind the scenes.Aggressive metrics: Corporate offices often push strict key performance indicators (KPIs) and production quotas on doctors and hygienists. If the staff suddenly seems overly aggressive about diagnosing extra procedures or recommending specific localized antibiotics, they may be trying to hit corporate thresholds.Understanding your rights as a patientYou are never completely powerless, even if your trusted dentist decides to sell the practice or abruptly quits. You hold fundamental rights regarding your dental and medical care:You own your healthcare dataA practice cannot withhold your records. You have the right to request full copies of your dental charts, x-rays, and treatment history at any time. The office is allowed to charge a nominal processing fee, but they cannot block access to your information.You have the right to a second opinionYou are never permanently locked into a single treatment plan. If a new dentist takes over your case and diagnoses expensive work you are unsure about, you are completely free to seek an outside opinion from an independent provider.You maintain the right to leaveIf the environment or treatment recommendations change in a way that makes you uncomfortable, you have the right to walk away. While getting a refund on pre-paid multi-year treatments like braces can sometimes be complicated, you are never forced to stay under corporate care.Understanding how your local office is owned helps you advocate for your health and choose the exact style of care that fits your family.
Unmasking the Friendly Dentist Model: Is Your Local Practice Secretly Corporate?When you walk into your local dentist or orthodontist’s office, you expect the same familiar faces and the personalized care you have trusted for years. However, behind the scenes, a major shift is occurring across the dental and medical industries. Corporate private equity (PE) firms are quietly buying up independent practices while keeping the original doctor’s name on the building.This strategy is known as the friendly dentist model. It allows corporate entities to take over operations without alerting patients who value local, independent healthcare.Signs your dentist might be secretly corporateBecause private equity firms try to make these transitions invisible, you have to look closely to see if your practice has changed hands.Website footers: Scroll to the absolute bottom of your dentist’s website. Look closely for tiny print using phrases like “powered by,” “affiliated with,” or “partners of” followed by a corporate name.Generic online portals: If the online booking links, digital intake forms, or bill payment portals suddenly look highly generic and unbranded, it might be a standardized corporate platform.High staff turnover: Private equity takeovers often introduce new compensation structures that cause long-term staff to leave. If you notice a steady trickle of new faces at the front desk and in the back office, the culture may have shifted behind the scenes.Aggressive metrics: Corporate offices often push strict key performance indicators (KPIs) and production quotas on doctors and hygienists. If the staff suddenly seems overly aggressive about diagnosing extra procedures or recommending specific localized antibiotics, they may be trying to hit corporate thresholds.Understanding your rights as a patientYou are never completely powerless, even if your trusted dentist decides to sell the practice or abruptly quits. You hold fundamental rights regarding your dental and medical care:You own your healthcare dataA practice cannot withhold your records. You have the right to request full copies of your dental charts, x-rays, and treatment history at any time. The office is allowed to charge a nominal processing fee, but they cannot block access to your information.You have the right to a second opinionYou are never permanently locked into a single treatment plan. If a new dentist takes over your case and diagnoses expensive work you are unsure about, you are completely free to seek an outside opinion from an independent provider.You maintain the right to leaveIf the environment or treatment recommendations change in a way that makes you uncomfortable, you have the right to walk away. While getting a refund on pre-paid multi-year treatments like braces can sometimes be complicated, you are never forced to stay under corporate care.Understanding how your local office is owned helps you advocate for your health and choose the exact style of care that fits your family.
What Your Dentist Knows About Your Health (And What They Can’t Say)
When you sit in the dental chair and open wide, you might think your dentist is only looking for cavities or checking how well you brush. But your mouth acts as a powerful window into your entire body. In fact, dental professionals can spot subtle clues about your systemic health, lifestyle choices, and even long-term longevity risks long before you ever experience symptoms elsewhere.However, the connection between oral health and medicine is complicated. Because of how the dental profession is regulated, primary care dentists often operate with strict legal and insurance limitations regarding medical diagnoses. If your dentist drops a subtle hint or nudges you to see your primary care physician, you should take it seriously—they often see more than they are legally allowed to explicitly say.Cardiovascular Risk and InflammationOne of the most clear-cut systemic signs a dentist can spot is cardiovascular risk.When a patient presents with severe gum disease (periodontitis) that doesn’t align with the amount of plaque in their mouth, it signals a deeper systemic problem. Pathogenic oral bacteria, such as Porphyromonas gingivalis, can enter the bloodstream through inflamed, bleeding gums. Once in the blood, these bacteria trigger low-grade systemic inflammation. This response elevates acute-phase proteins like C-reactive protein (CRP) and cytokines, which are heavily linked to atherosclerosis and a significantly higher risk of heart attacks.Uncontrolled DiabetesThe relationship between diabetes and periodontal disease is a well-documented, dangerous two-way street.Chronic high blood sugar levels physically alter the microvascular network—the small blood vessels—inside your gums. This impairment prevents your body from efficiently delivering essential immune cells to fight off standard oral bacteria. As a result, individuals with undiagnosed or poorly managed diabetes often experience rapid, severe bone and tissue loss around their teeth. The structural housing holding the teeth literally falls apart, leading to loose teeth that may eventually require extraction. Simply cleaning the teeth will not fix this; the systemic blood sugar must be addressed.Sexually Transmitted Infections (STIs)Dentists and orthodontists frequently identify signs of various STIs localized within the oral cavity. They routinely spot lesions, white patches, or sores related to:HPVSyphilisHIVHerpes Simplex Virus (HSV)Identifying these conditions requires extreme medical delicacy and privacy, particularly when treating patients under the age of eighteen where practitioners act as mandated reporters. While severe or rough oral physical trauma leaves distinct markers, it is worth noting that viruses like herpes are not exclusively transmitted sexually; they can easily be passed to babies through simple, non-sexual contact like a kiss.Anemia and Nutritional DeficienciesYour dentist can immediately evaluate the vitality of your soft tissues to check for nutritional health.For instance, pale gums or a smooth, “bald” tongue (where the normal texturing sloughs away) are primary visual red flags for anemia. This condition is usually driven by severe underlying nutritional deficiencies, specifically low iron, vitamin B12, or folate levels.Chronic Stress and Medication UseThe exact consistency and volume of your saliva tell a deep story about your lifestyle and psychological state.Thick, stringy saliva or overly sticky oral tissues often point to elevated cortisol levels caused by chronic anxiety, trauma, or long-term career burnout. Alternatively, changes in saliva consistency frequently reveal hidden medication lists or lifestyle habits not disclosed on a medical intake form—such as the regular use of cannabis, GLP-one weight-loss medications, SSRI antidepressants, or nicotine pouches.Oral Frailty and LongevityUltimately, your mouth serves as an accurate systemic biomarker for your total life expectancy.Prospective cohort studies examining the aging process demonstrate that oral frailty—specifically losing five or more teeth by age sixty-five—strongly correlates with significantly higher all-cause mortality rates. While losing a tooth does not directly cause death, a mouth that is structurally falling apart is a reflection of poor nutritional intake, long-term systemic inflammation, and lower socioeconomic wellness.The Tricky Position of the Modern DentistEven though your dentist can easily spot the oral warning signs of liver disease, kidney issues, or metabolic failure, they generally cannot order blood work or diagnose these medical conditions outright.Because doing so could expose them to liability or violate state dental board regulations, many dentists choose to stay quiet or offer vague advice. A new wave of functional medicine certifications for dentists aims to bridge this gap in the future. Until then, if your dental provider suggests that you follow up with a physician, do not ignore it—be completely candid with them and take proactive care of your systemic health.Disclaimer: This article is for general informational purposes only and does not constitute medical or dental advice, diagnosis, or treatment. Always consult with your own licensed healthcare provider regarding any medical conditions.
Is the Profession of Orthodontics Going Extinct? Should You Specialize?
 Is the Profession of Orthodontics Going Extinct? Should You Specialize?
Is the Profession of Orthodontics Going Extinct? Should You Specialize?
I. Introduction
Dr. Amanda from StraightSmile Solutions delivers a candid take: orthodontics as a specialty is facing extinction within her lifetime, not fully, but significantly.
More orthodontists are being produced than needed, while GPs and pediatric dentists are increasingly doing ortho.
If given the choice again, she would not specialize in orthodontics, and she advises others against it.
II. Why the Shift?
Traditional orthodontics addresses symptoms (crooked teeth) rather than root causes (poor facial development, airway, posture).
Waiting until age 10–12 means missing the growth window – 60% of facial growth is complete by age 6, 80% by age 8.
Insurance‑driven models and corporate DSOs profit from waiting until development fails, then selling mechanical solutions (braces/aligners).
Residency programs do not prioritize interceptive growth, airway, or early pediatric intervention because the business model is built on backend treatment.
III. The Preventive Alternative
If we focus on early intervention – nasal breathing, posture, diet, myofunctional therapy – the vast majority of children would never need braces (cosmetics aside).
True craniofacial orthopedics is about preventing structural failures, not hiding them behind a straight smile.
Functional issues should be addressed early (age 2–5), not at age 10 when growth is nearly complete.
IV. The Current Landscape
Orthodontists are unhappy; the system is not working.
Pediatric dentists and GPs who adopt early interceptive models are thriving (cash‑pay, fee‑for‑service).
However, the current insurance model does not pay adequately for the pre‑work (Phase 1) – it pays for Phase 2.
The solution: shift to fee‑for‑service and medicalize early airway/orthopedic care.
V. What This Means for You
If you are considering specializing in orthodontics, think twice.
The future belongs to primary care dentists who learn early interceptive growth guidance.
Dr. Amanda is building a West Coast team (ENT, OMT, pediatric dentists) focused on airway and growth – not traditional tooth straightening.
She recommends courses by Dr. Simon Long (removables) and her own (Invisalign/fixed) – and is open to collaboration with like‑minded clinicians.
VI. The Bottom Line
Traditional orthodontics is becoming obsolete. The old model of waiting, extracting, and mechanically aligning teeth is being replaced by early, preventive, growth‑guided care.
The money and satisfaction are in Phase 1 interceptive treatment and airway management, not in routine braces.
Specializing in orthodontics is no longer a safe bet. Instead, learn to grow faces, not just straighten teeth.