StraightSmile Solutions®
Are you REALLY an Airway Orthodontist?

I. Introduction
- Brief introduction to the concept of airway orthodontics
- Introducing Dr. Amanda from StraightSmile Solutions
- Purpose of the article: To discuss five crucial questions for dentists and orthodontists to assess if they are practicing airway orthodontics effectively
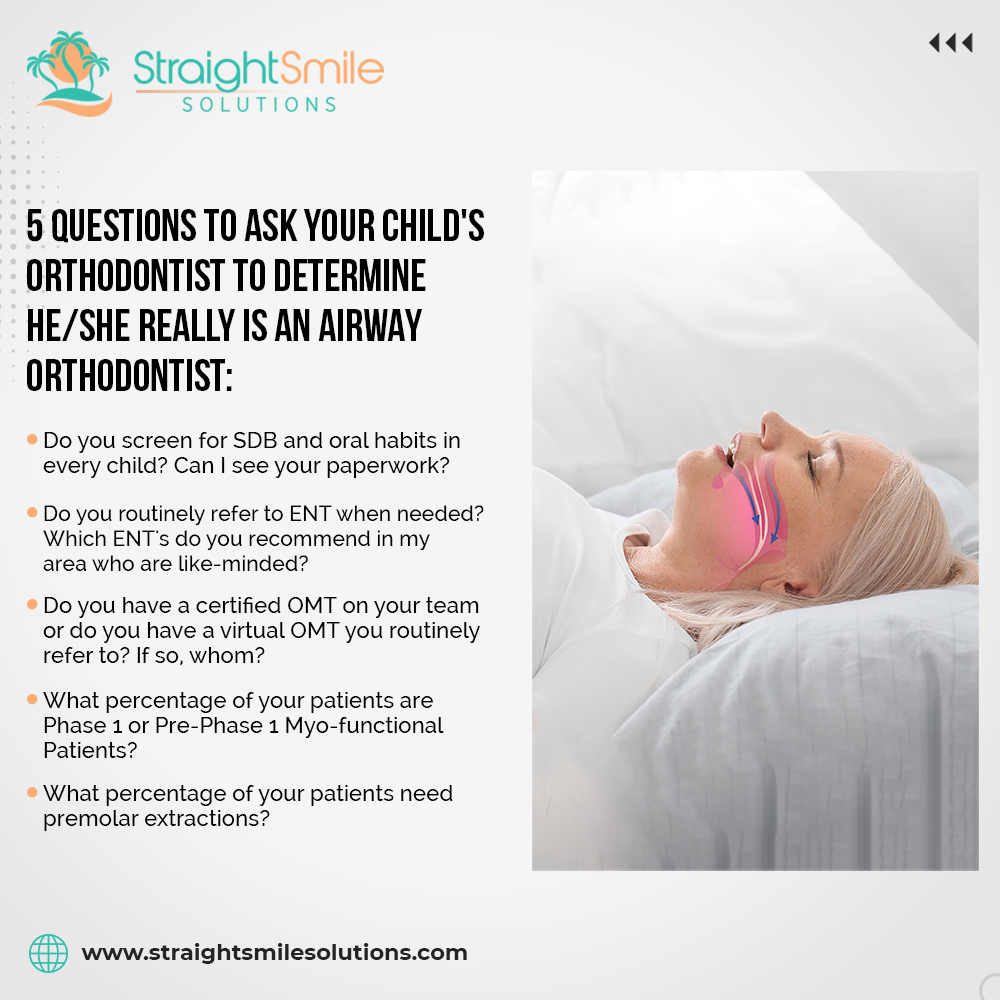
II. Screening for Sleep-Disordered Breathing (SDB)
- Importance of screening for SDB in every child
- Significance of oral habits and SDB forms
- Timing and accuracy of SDB screening
- Emphasizing the need for thorough parental involvement
III. Documentation and Referrals
- Importance of proper paperwork in airway orthodontics
- Utilizing effective SDB and oral habits forms
- Establishing referral pathways to Ear, Nose, and Throat (ENT) specialists
- Building collaborative relationships with like-minded ENT professionals
IV. Incorporating Orofacial Myofunctional Therapy (OMT)
- Essential role of certified OMT professionals in the team
- Importance of routine referral to OMT specialists
- Emphasizing the need for consistent utilization of OMT in treatment plans
- Avoiding sporadic or insufficient referrals to OMT specialists
V. Early Intervention and Phase One Treatment
- Significance of early intervention in airway orthodontics
- Identifying candidates for phase one or pre-phase one myofunctional therapy
- Assessing the percentage of patients receiving early intervention
- Avoiding delayed intervention for better treatment outcomes
VI. Minimizing Premolar Extractions
- Assessing the necessity of premolar extractions in treatment plans
- Evaluating the patient demographics and treatment approach
- Red flags associated with excessive premolar extractions in children and teens
- Considering alternative treatment modalities for optimal outcomes
VII. Conclusion
- Recapitulation of the importance of airway orthodontics
- Dr. Amanda’s insights and recommendations for dental professionals
- Encouragement to implement changes for enhanced patient care and outcomes
- Acknowledgment of the evolving landscape of orthodontic practices and the need for continual improvement
VIII. Closing Note
- Expressing gratitude for the readers’ attention
- Invitation to engage in further discussions and learning opportunities
- Wishing success and growth in the journey towards airway-centric orthodontic practices
- Contact information from Dr. Amanda for further inquiries or consultations
5 Things I Don’t Like about Invisalign Expanders

I. Introduction
- A brief overview of Dr. Amanda from StraightSmile Solutions‘ perspective on the new Invisalign expander.
- Introduction to the five concerns raised regarding the expander.
II. Cost: A Major Concern
- Discuss the exorbitant cost of the new expander and contrast it with other available options.
- Exploration of the expectation that it would be bundled with comprehensive plans and the disappointment in the additional fee.
III. Vertical Control: Limitations and Concerns
- Analysis of the expander’s limitations in modifying the vertical aspect, particularly its unsuitability for patients with short faces.
- Comparison with traditional expanders that offer more control over the vertical dimension through acrylic modifications.
IV. Habit Control: The Need for Flexibility
- Examination of the absence of customizable options for habit control in the new expander.
- Critique the potential impact of excessive acrylic on tongue position and its implications for habit correction.
V. Lack of Lower Expansion Integration: Missed Opportunities
- Discussion on the importance of simultaneous upper and lower expansion for optimal results.
- Disappointment in the inability to incorporate lower expansion simultaneously with upper expansion or aligner treatment, without paying an additional fee for Invisalign First Lab Fee. Also, this isn’t offered with Invisalign Comprehensive.
VI. Lack of Multitasking: Efficiency Concerns
- Exploration of the new expander’s lack of multitasking capabilities leads to potential inefficiencies and patient dissatisfaction.
- Advocacy for clearer educational resources and training modules to accompany the release of the expander.
VII. Conclusion
- Recap of the five concerns raised regarding the new Invisalign expander.
- Call for further education and clarification from Align Technology to address these concerns and ensure successful integration into orthodontic practices.
VIII. Additional Comments
- Open invitation for further discussion and insights from readers.
- Acknowledgment the need for ongoing dialogue and clarification regarding the new expander’s functionality and integration into clinical practice.
Are you REALLY an AIRWAY DENTIST?
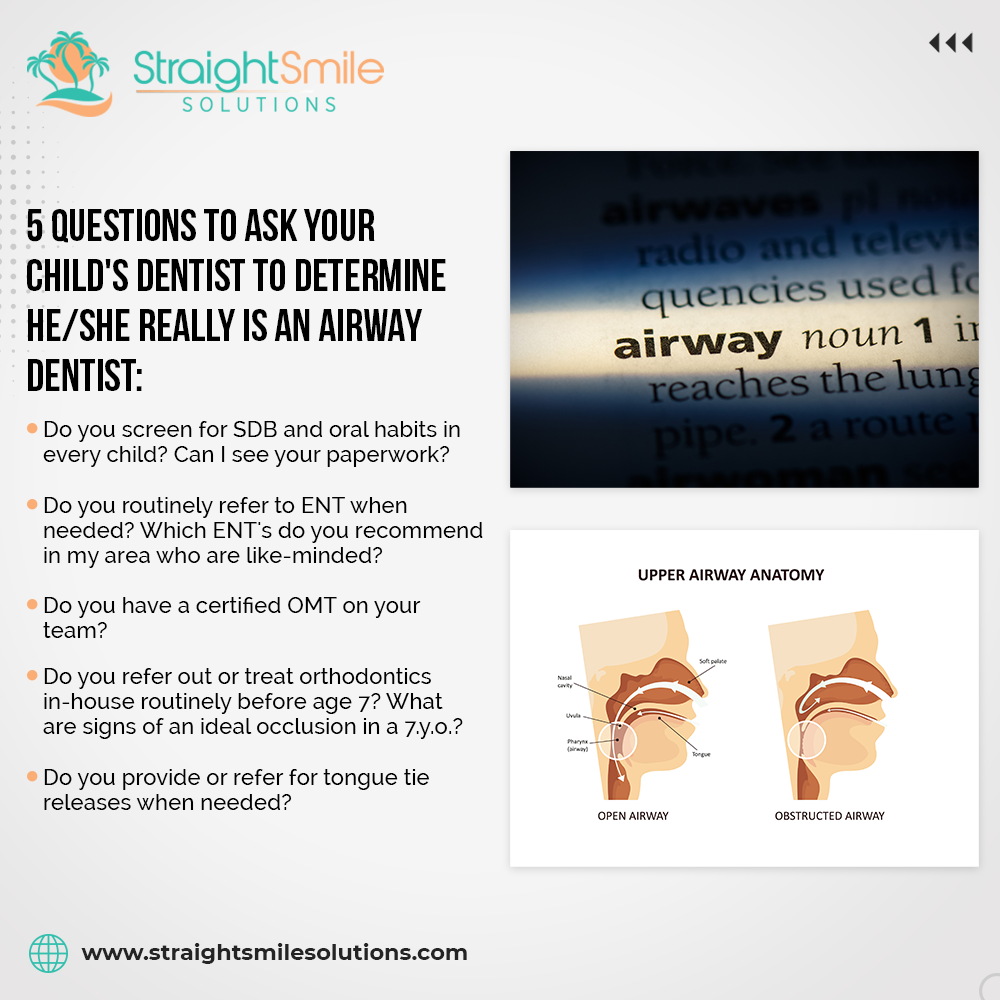
Are you REALLY an AIRWAY DENTIST?
Introduction:
● Dr. Amanda introduces the importance of airway health in dentistry.
● The significance of being an airway-focused dentist in today’s informed patient population.
● Overview of the five key questions to determine if a dentist is truly airway-focused.
1. Do You Screen for Sleep-Disordered Breathing (SDB) and Oral Habits?
● Explanation of the importance of thorough screening for SDB and oral habits.
● Emphasis on providing parents with screening forms to observe their child’s behavior.
● Recommendation of specific screening tools such as the FARES form.
● Importance of actively engaging parents in the screening process.
2. Do You Routinely Refer to ENT When Needed?
● Discussion on the necessity of collaborating with Ear, Nose, and Throat (ENT) specialists.
● Criteria for determining when referrals to ENT are necessary.
● Importance of building relationships with like-minded ENT specialists.
● Consideration of alternative diagnostic tools such as cephalometric analysis.
3. Do You Have a Certified Orofacial Myofunctional Therapist (OMT) on Your Team?
● Explanation of the role of Orofacial Myofunctional Therapy in airway-focused dentistry.
● Benefits of having a certified OMT on the dental team.
● Alternatives such as working with virtual OMTs.
● Strategies for integrating myofunctional therapy into dental treatment plans.
4. Do You Refer Out or Treat Orthodontics In-House Before Age Seven?
● Explanation of the importance of early orthodontic intervention for airway health.
● Discussion on the limitations of waiting until age seven for orthodontic assessment.
● Strategies for early intervention including monitoring, habit cessation, and referral to specialists.
● The importance of educating parents about the significance of early orthodontic treatment.
5. Do You Provide or Refer for Tongue Tie Releases When Needed?
● Overview of the role of tongue ties in airway health.
● Discussion on the judicious approach to diagnosing and treating tongue ties.
● The importance of offering or referring for tongue tie releases when appropriate.
● Consideration of alternative treatments and interdisciplinary collaboration.
Conclusion:
● Recap of the importance of airway-focused dentistry in promoting overall health.
● Encouragement for dentists to reflect on their practice’s approach to airway health.
● Reminder of the five essential questions to ensure a practice is truly airway-focused.
● Call to action for dentists to prioritize airway health in their practice for the benefit of their patients’ well-being.
How Your Patient’s Eyes Can Hint At Orthodontic Issues
How Your Patient’s Eyes Can Hint At Orthodontic Issues
Before a patient’s ortho starts, considering whether there are any “warning signs” is highly important. However, one factor you may not have thought to look at is the eyes. After all, it doesn’t really seem like the eyes will necessarily be relevant for orthodontics cases; however, they can provide useful information that may help. As such, today, we’re looking at how the eyes can help before ortho starts to help you choose an effective treatment plan.
How Can The Eyes Be Relevant in Orthodontics Cases?
There’s a good chance you don’t spend much time studying a patient’s eyes before ortho starts, but this could leave you missing out. Indeed, the eyes can provide useful info on several things, including breathing, sleep disorders, airway issues, or malocclusion. As such, checking them carefully may prove useful.
Some common signs are shiny eyes or Venus Pooling (dark and puffy circles under the eyes). These can be caused by several factors, and may be compounded when the patient has an underdeveloped midface or retrognathic jaws (i.e., a small SNA).
Another sign is sclera showing more prominently than you might expect. This could be due to a habit or certain diseases, but this can also suggest a lack of midface or jaw development, increasing the risk of poor airways.
Don’t Rule Out Other Causes
While we’ve looked at how the eyes could potentially indicate airway issues and the like in your orthodontics patients, it’s worth noting that these signs could come about for a few reasons. However, if you notice these consistently in a patient, it may be worth looking into this.
How to Turn your Dental Office to a Med Spa on Off Days

How to Turn your Dental Office to a Med Spa on Off Days
Introduction:
Meet Dr. Amanda, a dental professional with StraightSmile Solutions; today, she delves into transforming your dental office into a med spa. In this insightful discussion, Dr. Amanda addresses the growing trend of incorporating injectables like fillers and neurotoxins into dental practices. While emphasizing her non-affiliation with the discussed company, Cloud Med Spa, Dr. Amanda sheds light on a TurnKey approach offered by the company. Cloud Med Spa provides a comprehensive package, including software, product access, and the option for dental professionals to become injectors. Dr. Amanda highlights the potential benefits, such as additional revenue streams, increased foot traffic, and collaborative opportunities. Intrigued? Reach out to Dr. Amanda for more details on this innovative venture.
Section 1: The Untapped Potential for Dentists in Med Spa Services
● Recognition of dentists already offering injectables (fillers and neurotoxins) but often in an unsophisticated manner.
● Dr. Amanda’s curiosity was sparked by an orthodontic podcast discussing turning offices into med spas.
● Addressing the question of why general and pediatric dentists are not widely aware of this opportunity.
● Encouragement for dentists to explore the legal aspects of offering therapeutic and cosmetic neurotoxins in their state.
Section 2: Introducing Cloud Med Spa’s TurnKey Approach
● Introduction to Cloud Med Spa’s TurnKey approach and its potential benefits.
● Explanation of Cloud Med Spa’s offering: providing assets to transform existing dental offices on non-dentistry days.
● Emphasis on the additional revenue stream and increased foot traffic generated by aesthetic clients.
● Highlighting the potential for new patients to discover the dental services during their med spa visits.
Section 3: Understanding Cloud Med Spa’s Support
● Dr. Amanda’s commitment to sharing information learned from a recent call with Cloud Med Spa.
● Overview of the software, injectables, and neurotoxins provided by Cloud Med Spa to licensed dentists.
● Discussion on dentists’ role as injectors and the option to recruit RNs or physicians if they prefer not to be injectors.
● Clarification on the 1099 status of recruited RNs, emphasizing the flexibility of scheduling.
Section 4: Benefits and ROI of Cloud Med Spa
● Emphasis on the affordability of Cloud Med Spa’s services.
● Discussion on the potential return on investment, including revenue from rentals and product commissions.
● Pointing out the benefit of collective buying, reducing costs through crowdsourcing among participating dental offices.
● Highlighting the assistance provided by Cloud Med Spa in onboarding providers and managing vendor relationships.
Section 5: Additional Services and Conclusion
● Mentioning additional services such as preceptors, provider training, and vendor management.
● Acknowledging the strategic aspects of site management, software, and community building provided by Cloud Med Spa.
● Encouraging interested parties to contact Cloud Med Spa directly or reach out to Dr. Amanda for a direct referral.
● Reiteration of no financial incentives for Dr. Amanda and her enthusiasm for the potential of Cloud Med Spa.
Conclusion:
Dr. Amanda shares an intriguing opportunity for dental offices to venture into the world of medical spas with Cloud Med Spa. Emphasizing her lack of affiliation or financial incentives, she underscores the potential for dental practitioners already involved in injectables to optimize their space and increase revenue. The TurnKey approach offered by Cloud Med Spa provides software, product access, and a streamlined process for injecting services. With an affordable investment and the potential for significant returns, the initiative seems promising. Dr. Amanda highlights the benefits, from additional revenue streams to attracting new clients interested in both aesthetics and dental services. Interested practitioners are encouraged to reach out for more information, as Cloud Med Spa appears to offer a valuable and well-supported opportunity for dental offices.
Rapid vs Slow Turns with RPE and Schwartz
Rapid vs Slow Turns with RPE and Schwartz
When it comes to expansion cases, should you be using rapid or slow turns with RPE or Schwartz? There are benefits associated with both rapid and slow turns, and keeping this in mind is important to ensure that your orthodontics patient is fully aware of the process and that finishing cases is simple and low-risk.
The Challenges of Rapid Expansion
There are several potential orthodontics challenges with rapid expansion and turns in fixed cases, and this can make finishing cases comfortably and successfully difficult. One common issue is that patients who speak English as a second language may struggle to understand the rapid turns, which can lead to discomfort if they use too rapid turns. Additionally, in a handful of rare cases, there is a risk of excessively rapid turns being used as a punishment.
Benefits of Slow Turns
Slow turns can make finishing cases in orthodontics much slower, but there are numerous benefits associated with this. For one thing, this allows you to keep the same instructions for both removable and fixed expansion cases, regardless of whether you use RPE or Schwartz; this makes instructions much more consistent.
Slow turns can also lead to fewer risks and complications, while also preventing the large gap between the front teeth that can arise with rapid turns. This also helps provide gentle, more comfortable alignment.
Don’t forget, with slow turns especially, make sure you get the patient in regularly to check the frequency. In addition, all expander patients should have an appointment to follow up; never ghost an expander patient, as strange things can potentially happen.
Managing Second Opinions in Orthodontics Cases
Managing Second Opinions in Orthodontics Cases
In some cases, patients may seek a second opinion for their orthodontics treatment plans, and knowing how to tackle these cases is highly important to help inform your approach to second opinions in orthodontics cases. As such, we’ve outlined some key things you should know about second opinions as follows to help.
The Two Types of Second Opinions in Orthodontics
Getting involved with second opinions can be risky. Generally speaking, you may not want to give second opinions on other providers’ treatment plans and pricing, as everyone has their own approach to treatment planning, training, pricing, and the like.
You should always stick with the treatment plan and price point you are most comfortable with, and informing the patient of this is usually safe. However, you should avoid giving feedback on another doctor’s treatment plan or pricing directly, as this can lead to contentions and issues arising with the other provider. Ideally, don’t even look at the other provider’s notes to avoid potential liabilities.
Second Opinions on Consults
When patients come to you looking for a second opinion on a consult, they usually want either a better price or a different treatment plan. These consults are much like regular orthodontics consultations and you should treat them as such; however, don’t give feedback (especially not negative feedback) on someone else’s opinion to avoid getting into hot water.
Second Opinions on Orthodontic Work
If a patient comes into your office having already received orthodontic work, or if one of your patients who’s had ortho from your clinic seeks a second opinion, this can potentially be risky. Be very careful how you address these second opinion cases to avoid criticizing the other orthodontist.
In any case, you should never give a second opinion based on the patient’s statements alone; always make sure you have full records of the progress notes, treatment plans, and so on first, such as the ceph and panoramic X-rays. Moreover, if your patient visits another orthodontist for a second opinion, make sure you offer to support with any concerns they may have, in case this has cause them to approach someone new.
Invisalign Pay as you go Refinements in Australia
Invisalign Pay as you go Refinements in Australia
I. Introduction
Dr. Amanda discusses a new “pay as you go” refinements feature that Invisalign has launched in Australia. She is very excited about this as it provides significant savings for doctors and patients. She also financially incentivizes doctors to plan cases properly and ensure patients track properly to avoid needing refinements. The savings are substantial – the unlimited refinement plan is now AUD 1,400 cheaper. She then discusses the types of cases suitable for the 4-year no-refinement option. She estimates that for the “right case,” one could pay a similar price as an Invisalign Lite case but with the potential for hundreds of aligners. She hopes this program comes to the U.S. and Canada as well.
II. Invisalign Pricing Overview in Australia
A. Historical pricing issues
1. High costs and reasons speculated
B. Introduction of pay-as-you-go refinements
1. Comprehensive feature pricing reduction
a. Five-year unlimited refinements now at $3,738 Australian
2. Four-year no-refinement option for skilled doctors
a. Criteria for the right case
i. Class one without periodontal disease
ii. No Bolton discrepancy
iii. Mild to moderate crowding or spacing
iv. No rotated pre-molars or molars
v. No IPR, sequential distalization, or MA advancement feature
3. List price for pay-as-you-go refinements at $2,418
a. Additional 10% off for the next quarter
4. Flexibility and value comparison
a. Up to four years to complete a case for $385 (including tax)
III. Case Analysis and Considerations
A. Selecting the suitable case for pay-as-you-go refinements
1. Doctor’s skill and treatment planning expertise
2. Criteria for the ideal case
a. Class one alignment
b. Absence of periodontal disease
c. No Bolton discrepancy
d. Mild to moderate crowding or spacing
3. Avoiding IPR and sequential distalization
a. Reduced chances of needing refinements
4. Value proposition for doctors and patients
IV. Speculation on Future Availability
A. Beta testing in Australia
B. Hope for the introduction in the U.S. and Canada
C. Incentivizing proper treatment planning
1. Financial motivation for doing things right
2. Potential impact on the frequency of refinements
V. Conclusion
Dr. Amanda’s enthusiasm for the new pay-as-you-go refinements with Invisalign in Australia is well-founded and contagious. The launch addresses the longstanding issue of high Invisalign prices in Australia, offering a revolutionary approach to comprehensive features. The reduction in cost for the five-year unlimited refinements feature, now at $3,738 Australian, is significant. Dr. Amanda emphasizes the value of this option for skilled doctors handling straightforward cases without complications like periodontal disease or Bolton discrepancies. Introducing a four-year no-refinement option further streamlines the process, encouraging precise treatment planning. The discounted list price of $2,418, with an additional 10% off for the next quarter, adds to the allure. Dr. Amanda’s optimism extends beyond Australia, hoping for a global implementation that could revolutionize Invisalign practices worldwide.
Using the Invisalign Apps on the App Store and the Google Play Store

Using the Invisalign Apps on the App Store and the Google Play Store
When it comes to Invisalign cases, being able to access the Invisalign app directly on your phone and use this effectively can be very helpful. However, there are many apps claiming to be Invisalign or for clear aligners, and it’s not always clear which app you need. As such, we’ve outlined some key things you should know as follows to help.
My Invisalign vs Invisalign Practice App: Which is Genuine?
To start with, it’s worth noting that there are two official Invisalign apps on the market: My Invisalign and the Invisalign Practice App. It’s easy to assume that one of these must be fake, but that’s not the case. In fact, these apps simply have different audiences.
The My Invisalign app is designed for patients to help guide them through their Invisalign journey. The patient app is incredibly well-received with hundreds of thousands of downloads and excellent reviews.
Meanwhile, as an orthodontist or a general dentist just starting out with orthodontics, you’ll want the Invisalign Practice App. Unfortunately, this app doesn’t have quite the same praise as the patient app, although it can offer useful features.
Should I Use the Invisalign App?
You don’t necessarily need to use the Invisalign app, but there are certain features that are exclusive on the app. For example, the photos system offers a range of unique features, so this is worth considering as an option for your orthodontics cases.
How to Treatment Plan Class II, Div II Growing Kids in Stages

How to Treatment Plan Class II, Div II Growing Kids in Stages
Have you ever wondered about how to treatment plan for kids with a Class 2, Div 2 malocclusion in stages? Knowing how to approach these different cases in your orthodontics treatment plans is highly important; luckily, our team here at Straight Smile Solutions can help.
As such, we’ve outlined some key things as follows to help you create an effective orthodontics treatment plan for Class 2, Div 2 growing kids; alternatively, contact us to book your own A La Carte session with our team for support.
How to Treatment Plan for Class 2, Div 2 Growing Kids
With Class 2, Div 2 growing kids, you’ll often see that the incisors are retroclined, which results in a hidden overjet of up to 9mm. However, sometimes with these cases (and this isn’t necessarily predictable), the lower jaw may grow if it still has growth potential, especially if you have simultaneously advanced the lower jaw.
As such, when making a treatment plan, be careful not to create a full treatment plan, as there is the potential that the orthodontic requirements may change.
When tackling Class 2, Div 2 cases with Invisalign with MA, you’ll usually find that they straighten the teeth initially, and the MA component only begins around halfway through the treatment plan. Similarly, if you are doing braces or expanders in Class 2, Div 2 patients, you’ll need to use the same approach.
As such, when starting out with these cases, it’s potentially worth starting with a little expansion (if they are constricted), before using a few top braces and seeing how things progress. The patient’s progression from this point will then influence how you tailor the treatment plan for their needs; you may find that this initial step is enough to trigger jaw growth alone, which is why it is not necessarily suitable to make a full treatment plan before ortho starts.