StraightSmile Solutions®
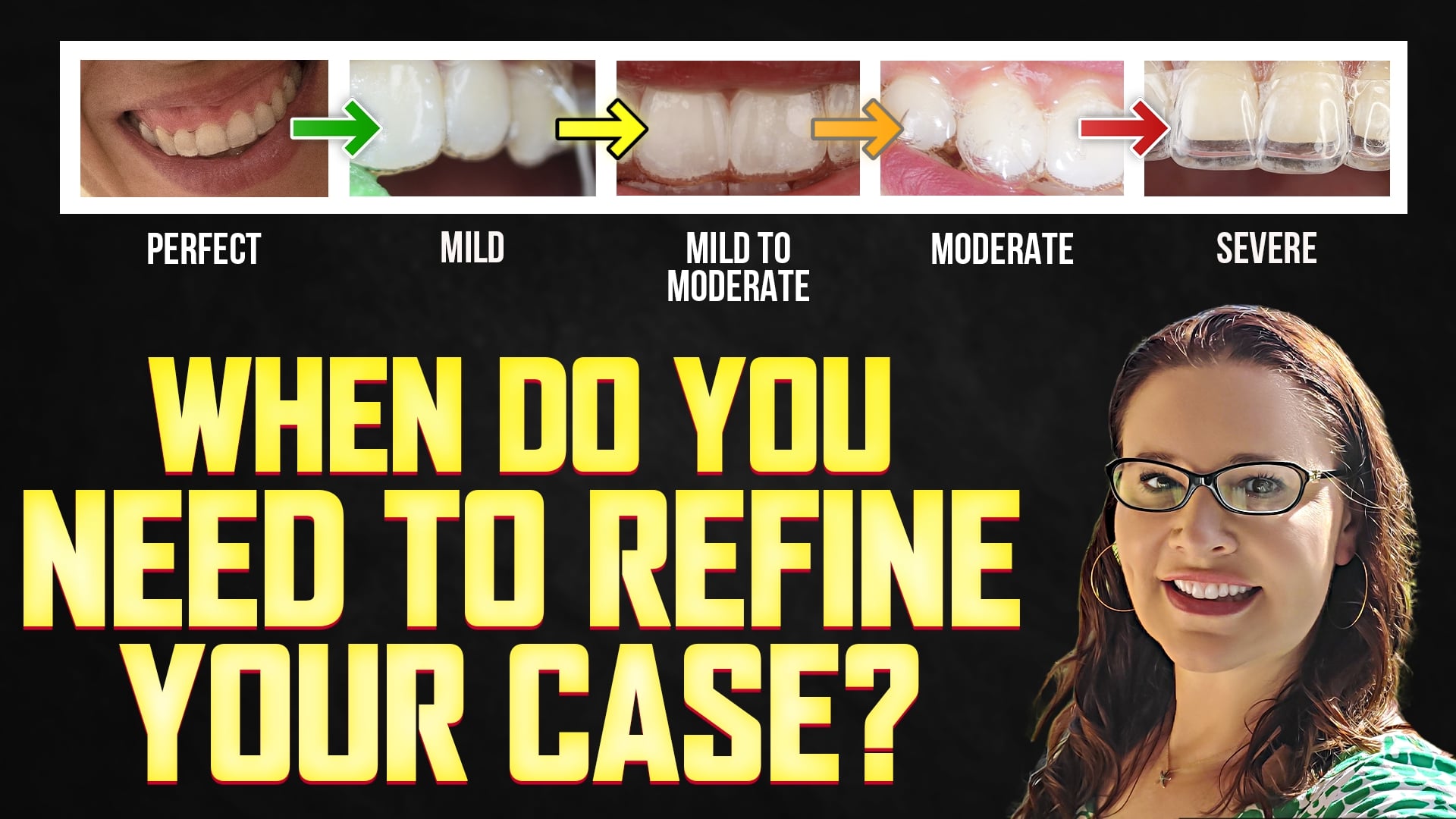
ONLY A MINOR TRACKING ISSUE? HOW TO MAKE INVISALIGN REFINEMENTS EASIER
- Understanding Minor Tracking Issues
• Minor tracking issues are common and not necessarily alarming if there’s no pathology and the bite remains stable.
• When issues arise, reboot the case to the original plan—no need for major changes unless problems worsen.
• Clinicians are advised against trying to “push through” misaligned cases with more aligners; this may cause complex setbacks.
• Do not appease patients by giving too many trays—limit to five until tracking improves.
• Virtual or in-person monitoring every few weeks is critical to catch and manage issues early. - Efficient Refinement Submission Tips
• Use existing attachments if they’re intact and well-placed—avoid unnecessary removal and re-bonding.
• Select “continue towards achieving the same final treatment plan” during submission to avoid resetting the whole case.
• Avoid the “make finishing adjustments” option, as it often derails previously optimized setups.
• Always review revised plans closely—even with proper selections, Invisalign may introduce unintended IPR or attachment changes.
III. Custom Treatment Instructions for Refinement
• Sample instructions include:
- “Use existing attachments unless replacement is necessary.”
- “Add additional attachments as needed for extrusions, torque, or rotations.”
- “Refer to movements in the previous plan.”
- “Finish with 3-point molar, 2-point premolar, and light canine guidance.”
• Inform the lab if IPR has already been completed to avoid repetition or under correction.
• Always count trays and estimate based on prior usage to avoid short refinements.
- Clinical Strategy for Success
• A strong initial ClinCheck, tight tracking oversight, and saved aligners allow for smooth reboots.
• Refrain from giving all trays at once unless systems are in place for accountability.
• Establishing refined workflows reduces the need for ongoing consultation and saves long-term time.
TOP RETENTION MISTAKES DOCTORS MAKE BEFORE DELIVERING ESSIX OR VIVARA RETAINERS
TOP RETENTION MISTAKES DOCTORS MAKE BEFORE DELIVERING ESSIX OR VIVARA RETAINERS
- Introduction: Addressing Retention Concerns
- Dr. Amanda responds to a viewer’s question regarding discomfort with a Vivara retainer, highlighting the importance of post-orthodontic care.
- The issue raised—pressure on a specific tooth from the retainer—illustrates common retention challenges.
- Retention is described as the third, often neglected, phase of orthodontic treatment.
- Dr. Amanda emphasizes that successful orthodontics doesn’t end with braces or aligners; it includes lifetime retention planning.
- The Importance of a Retention Protocol
- Many dental professionals overlook or inadequately address long-term retention.
- Dr. Amanda asserts that retention is both a patient satisfaction opportunity and a revenue stream.
- Poor retention planning leads to frustration, negative reviews, and missed referrals.
- A well-maintained outcome turns patients into “walking, talking billboards” for your practice.
III. Retainer Awareness Among Families
- Parents and teens frequently discuss retainer types and protocols in everyday settings (sports events, parks, etc.).
- Being transparent and informative about aftercare distinguishes dental providers and builds trust.
- Orthodontists are more likely than general dentists to have robust aftercare plans in place.
- Creating a Comprehensive Retention Plan
- Dr. Amanda recommends that all practices implement a clear, signed retention agreement before treatment begins.
- You should detail: type and number of retainers, replacement process, breakage protocols, and cost expectations.
- Should address relapse scenarios and future retainer needs.
- Outsourcing retainers to third parties may reduce long-term practice value; in-house management is preferred.
- Practice Growth and Support
- Dr. Amanda offers dentists a complimentary consulting session (not for case review) to explore retention strategies and services.
- Encourages participation in courses or à la carte support for deeper retention protocol implementation.
- Emphasizes hands-on learning and consistent access to professional guidance for retention success.
- Conclusion
- Retention is a critical but often neglected component of orthodontic success.
- Establishing a solid, transparent retention plan improves outcomes, reduces risk, and strengthens a practice’s reputation and longevity.

HOW TO ADD A PANO AT REFINEMENT WHEN ROOT UPRIGHTING IS A PROBLEM IN INVISALIGN
 HOW TO ADD A PANO AT REFINEMENT WHEN ROOT UPRIGHTING IS A PROBLEM IN INVISALIGN
HOW TO ADD A PANO AT REFINEMENT WHEN ROOT UPRIGHTING IS A PROBLEM IN INVISALIGN
I. The Role of Panoramic X-rays in Refinements
• Panoramic X-rays (PANO) are crucial for monitoring root positions, resorption, and pathology during Invisalign refinements, especially in cases requiring root uprighting.
• ClinCheck currently lacks a direct option to upload a PANO during a refinement, only allowing CBCT uploads if CBCT was included in the initial submission.
• Dr. Amanda highlights this as a limitation and advocates for PANO inclusion as a standard of care.
II. How to Add a PANO at Refinement
• Use a creative workaround by uploading the PANO in one of the available photo slots—e.g., replacing the profile photo or another image if necessary.
• Include clear treatment notes: “Refer to PANO in the photo section. Please upright tooth #__ as shown.”
• Email the PANO directly to Align Technology ([email protected]) with the case number and timing, noting in ClinCheck: “PANO sent at [time]; please refer to PANO to upright [tooth number].”
• Without clear notes, Align won’t act on the PANO—AI doesn’t diagnose or plan, it follows clinician instructions.
III. Misuse of AI in Treatment Planning
• Many clinicians overly rely on engines or AI-based Flex Rx setups without reviewing or adjusting plans.
• Dr. Amanda stresses that AI is a tool, not a replacement for clinical diagnosis and planning.
• In legal cases or complaints, clinicians are held accountable for poor planning.
• Always review AI-generated plans critically; override errors like unnecessary IPR or expansion.
IV. Clinical Recommendations
• Take PANO updates every 6–12 months or more frequently if clinical signs suggest root issues.
• Guide Align Technology with explicit directions—AI should assist, not replace, your judgment.
• The extra step of including a PANO helps ensure accurate root positioning and minimizes long-term complications.
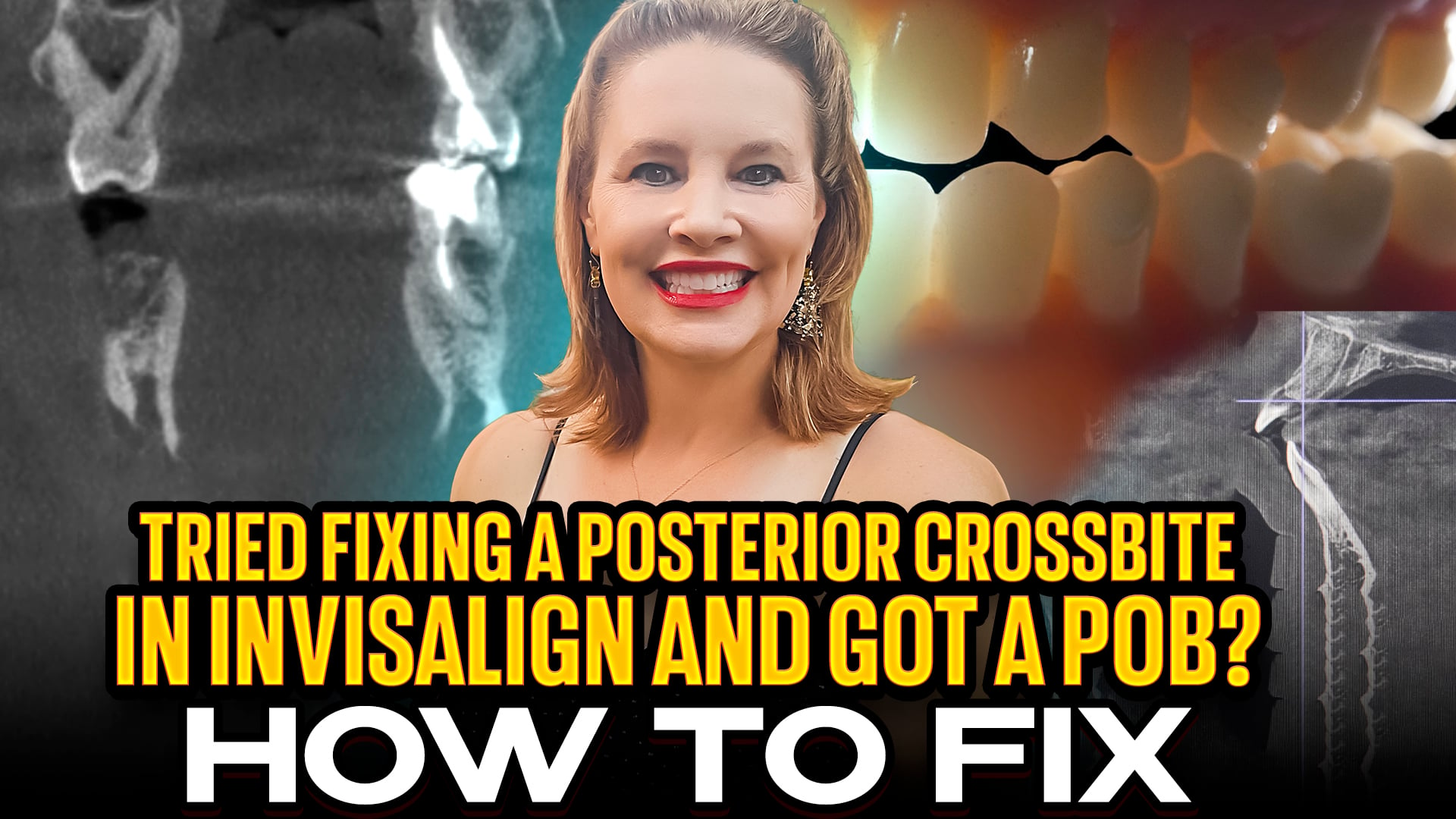
Crossbites and POBs – How to Fix in Aligners / Invisalign
- Introduction to Posterior Open Bites (POBs) and Crossbites
• Dr. Amanda from Straight Smile Solutions revisits the topic of posterior open bites (POBs) and posterior crossbites—common challenges in aligner orthodontics.
• POB = Posterior Open Bite; can be caused by vertical issues or arch expansion interferences.
• Emphasis on identifying the true cause—whether it’s vertical (bite opening due to intrusion/eruption) or transverse (due to arch shape or bone limitations).
• Aligners often fail to address these issues unless the underlying skeletal/bone anatomy is carefully considered.
• Planning errors (e.g., over-expanding or misdiagnosing the curve of Wilson) lead to complications that aligners alone cannot fix. - Diagnostic Tools: CBCT & Curve of Wilson Evaluation
• CBCT imaging is invaluable for planning, especially in adults, where bone stability is more predictable.
• CBCT-integration features (available in Invisalign and Spark) offer high-value insight, but not all platforms (e.g., Clear Correct) support it.
• Even if CBCT isn’t integrated, clinicians should examine transverse slices to evaluate bone presence and the Curve of Wilson shape.
• The Curve of Wilson (buccal-lingual inclination of molars) must be upright for proper occlusion—distortion leads to POBs.
• AI in aligner portals isn’t yet reliable for predicting bone response—manual assessment is essential.
III. Expansion Pitfalls and Treatment Planning
• Over-expansion is a common recommendation in ortho courses, but it’s not always safe.
• If the bone isn’t there, expanding the arch can push teeth out of the bony housing, creating instability and bite issues.
• Dr. Amanda warns that elastics or trimming trays cannot fix POBs caused by transverse interferences like an exaggerated curve of Wilson.
• Determining if the problem is skeletal vs. mechanical is the first step to effective planning.
• Clinicians must ask: “Can I expand?” “Is there bone?” “What’s happening with the Curve of Wilson?”
- Assessing Incisor Position & Bone Housing
• Flared incisors may already be outside the bony housing—further movement worsens the situation.
• Instead of flaring more, retraction might offer better stability and esthetics.
• CBCT or cephalometric images help confirm tooth position in relation to the alveolar bone.
• Important for making decisions about IPR, extractions, or avoiding over-expansion.
• Dr. Amanda emphasizes time-saving diagnosis: seasoned orthodontists can visually assess flared incisors without waiting for metrics.
- Conclusion and Clinical Takeaways
• Crossbites and POBs must be diagnosed correctly—vertical vs. transverse root causes.
• Use CBCT and assess the Curve of Wilson to avoid treatment failures.
• Aligners alone cannot fix biomechanical problems caused by poor planning or bone limitations.
• Utilize available tools and imaging to customize treatment, especially for complex cases.
• With accurate diagnostics and conservative biomechanics, clinicians can treat tougher cases safely and successfully.
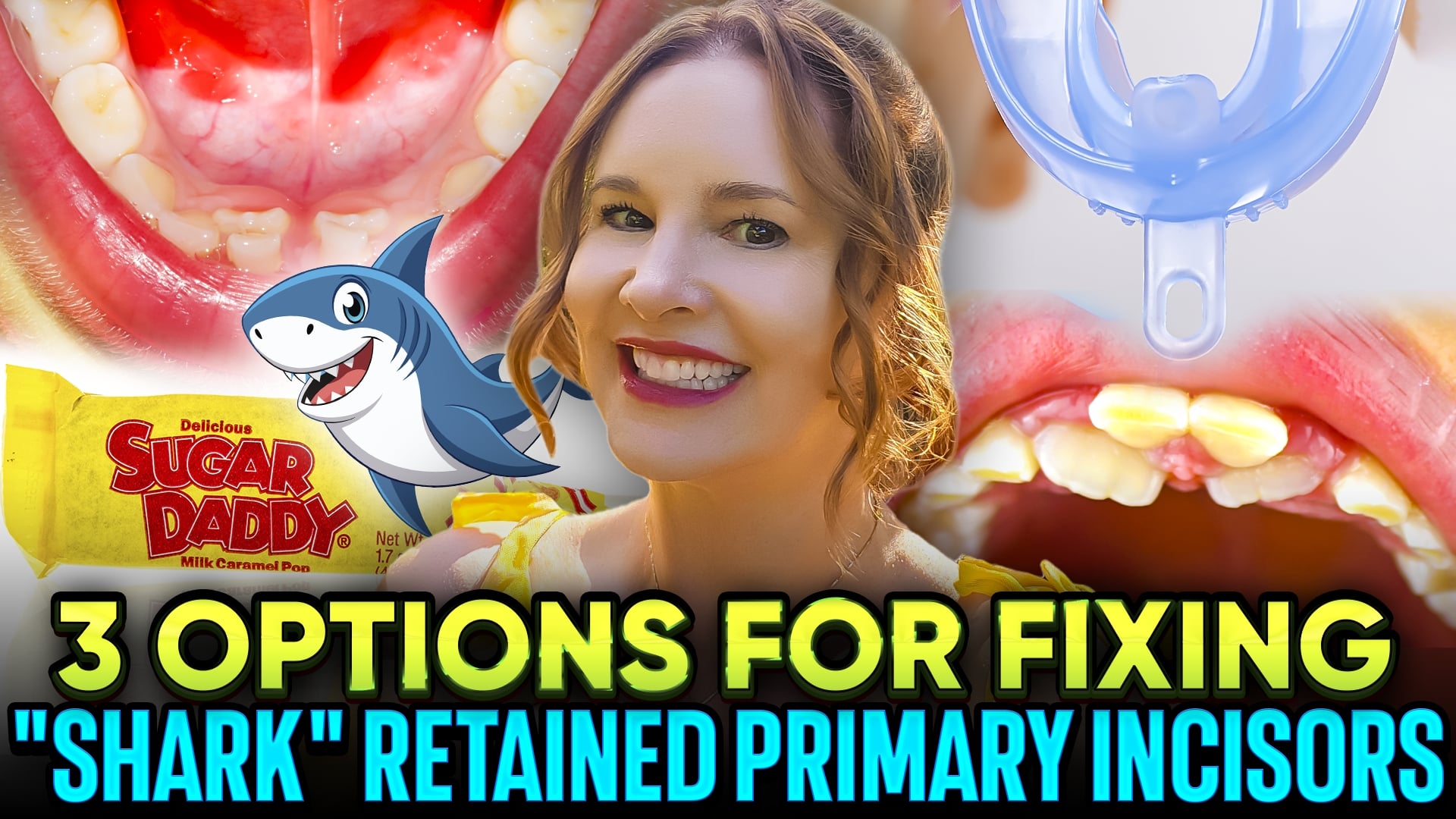
Non-Extraction Options for Shark-Retained Teeth
Non-Extraction Options for Shark-Retained Teeth
- Introduction
- Dr. Amanda from Straight Smile Solutions discusses “shark teeth,” a common condition where kids have two rows of teeth due to retained baby teeth.
- This occurs when the roots of baby teeth don’t resorb fully, often during the eruption of permanent incisors or molars.
- It’s a developmental variation—not always a cause for alarm.
- The key is understanding the child’s behavior (wiggler vs. non-wiggler) and family dynamics for appropriate treatment planning.
- Rushing into extractions isn’t always the best first step.
- Conservative Strategies for Shark Teeth
- Wiggling Encouragement: Children should be encouraged to manually loosen their baby teeth if they’re comfortable.
- Candy Orthodontics:
- Supervised biting of hard, sticky candies like Sugar Daddies helps dislodge retained teeth.
- Effective in children who can’t or won’t wiggle their teeth themselves.
- Must be paired with proper oral hygiene to prevent decay.
- These methods use natural muscle forces—what Dr. Amanda calls “free orthodontics.”
- Avoids trauma or complications of premature extractions.
III. Appliance-Based Support
- Bio-Trainers & U Concept Devices:
- Functional appliances that improve tongue posture, lip seal, and nasal breathing.
- Simultaneously help realign teeth and correct oral habits.
- Especially useful in sensory-sensitive children or when natural methods don’t work.
- These devices offer dual benefits: orthodontic support and improved orofacial function.
- Role of Parents & Hygiene
- Successful treatment depends on active involvement from both parents.
- Involving dads is essential—conflicts arise if only one parent consents.
- Hygiene is critical during the “shark teeth” phase.
- Tools like WaterPiks and Sonicare brushes help clean hard-to-reach areas.
- Especially important when candy, orthodontics, or appliances are used.
- Conclusion
- Most cases of shark teeth resolve without invasive procedures.
- Dentists should delay extraction unless infection, pain, or hygiene problems arise.
- Encourage natural loosening, involve both parents, and use tools like appliances or candy-based methods when needed.
- With proper supervision, children can benefit from their body’s natural mechanics to achieve healthy, aligned smiles.
Pediatricians are Missing the Ortho Referral Boat

- Introduction: Don’t Miss the Ortho Referral Boat
- Dr. Amanda from StraightSmile Solutions highlights how easily pediatric orthodontic referrals can be missed.
- Emphasizes the importance of follow-up, especially in phase one treatment, which can be completed quickly.
- Many general or pediatric dentists forget to revisit referrals, especially if they only see the patient once or twice per year.
- The Three Ages Every Child Has
- Every child has a chronological, skeletal, and dental age—these may not align.
- Especially relevant in female patients who may enter puberty early and develop out of sync.
- Ortho timing depends heavily on these developmental stages, not just the child’s age on paper.
III. Legal and Ethical Duty to Refer
- All dentists, regardless of specialty, have a legal responsibility to screen and refer for ortho.
- Even if not offering orthodontics, dentists must recognize when intervention is needed and continue referring if the patient doesn’t act.
- Qualified referrals include explaining risks, benefits, and alternatives of treatment.
- The Gap in Medical & Dental Provider Knowledge
- Many pediatricians and even dentists lack training in detecting airway and ortho issues.
- Dr. Amanda stresses that screening should extend beyond caries—look for airway concerns, crowding, and skeletal development.
- Pediatricians could benefit from even basic ortho training to improve early detection.
- Impact of Missed Timing—Especially for Girls
- Missing the puberty window often leads to substandard ortho outcomes.
- Some skeletal issues can’t be corrected later without surgery.
- Early screening can prevent complex interventions and improve airway and bite health.
- Dr. Amanda’s Call to Action
- Offers free and low-cost Phase 1 courses to help general/pediatric dentists.
- Advocates for this education to be taught in dental school and pediatric medical training.
- Announces a future removable appliance practice and seeks partners in pediatric dentistry.
Conclusion
- Early ortho screening is a shared responsibility across medical and dental fields.
- Proactive education and consistent referrals can save kids from lifelong dental and airway issues.
When to Add IPR Myo Appliances to that Aligner or Braces Case
 When to Add IPR Myo Appliances to that Aligner or Braces Case
When to Add IPR Myo Appliances to that Aligner or Braces Case
I Introduction & Diagnostic Priorities
• Dr. Amanda emphasizes the importance of diagnostics before initiating treatment for aligners or braces.
• Core focus: when to add IPR (Interproximal Reduction), myofunctional therapy (myo), or appliances.
• Customization based on patient-specific factors is critical; no one-size-fits-all approach.
• Tools like CBCT (Cone Beam CT) are highly recommended for advanced diagnostics.
II. Role of CBCT & Treatment Planning
• CBCT offers 3D insights into bones, teeth, and airway structures.
• Particularly valuable for planning aligner cases involving skeletal discrepancies or airway concerns.
• Not all aligner platforms (e.g., Clear Correct) integrate CBCT, but images can still guide treatment planning.
• Safe and effective use of CBCT helps prevent complications like posterior open bites (POBs).
III. Myofunctional Habits & Appliances
• Habits like thumb sucking, mouth breathing, and tongue thrusting can distort bites and facial growth.
• Myofunctional therapy may be necessary for long-term treatment stability.
• Appliances are sometimes required to address vertical, transverse, or airway-related issues.
• Expansion and crowding should be guided by bone availability—overexpansion leads to complications.
IV. Foundational Education & Resources
• Mastery of aligner therapy requires understanding phase one airway principles and straight wire basics.
• These principles guide decisions like whether to extract teeth, expand arches, or initiate myo therapy.
• Straight Smile Solutions offers CE courses and playlists tailored to orthodontic diagnostics and aligner planning.
V. Conclusion
• Successful orthodontic treatment blends diagnostics, technology, education, and habit management.
• Practitioners should leverage CBCT, address myofunctional issues, and stay educated to optimize outcomes.
• The video promotes a comprehensive, individualized approach to aligner and braces treatment.
The UGLY DUCKLING PHASE for Pediatric Phase 1 Interceptive Ortho
The UGLY DUCKLING PHASE for Pediatric Phase 1 Interceptive Ortho
- Introduction
- Amanda from StraightSmile Solutions explains the “Ugly Duckling Phase”—a normal and temporary stage of dental development.
- The “Ugly Duckling Phase” is a common, temporary stage in dental development.
- It typically occurs between ages 7 to 10 and is considered a positive sign of natural growth.
- While the term may sound harsh, it’s an affectionate orthodontic expression taught in dental school.
- What Is the Ugly Duckling Phase?
- Occurs during mixed dentition when permanent front teeth (incisors) erupt before the canines.
- The un-erupted canines push against the roots of the lateral incisors, causing the front teeth to tip outward.
- A midline gap or spacing between the front teeth is typical and expected.
- As the canines erupt, they naturally shift the incisors back into place, closing the space.
III. Why Parents Worry
- Parents often mistake spacing for orthodontic problems.
- In reality, this spacing is beneficial—it allows room for proper canine eruption.
- Crowding in this stage is more concerning than spacing.
- When to Monitor, Not Treat
- If a child is Class I around the arch, with good vertical and transverse development, spacing is ideal.
- Watch for:
- Habits (e.g., thumb sucking)
- Myofunctional issues
- Severe bite problems
- Lack of space (less than 6mm between incisors)
- Exceptions to Early Treatment
- Acting or modeling needs
- Severe self-esteem or psychosocial concerns
- Only in these cases may early braces be considered
- The Best Approach for Parents and Providers
- Avoid unnecessary treatment; most cases self-correct.
- Recommend six-month recall visits to monitor development.
- Communication is key—make sure both parents are on board if early treatment is chosen.
- Always prioritize ethical, patient-first care.
Conclusion
The “Ugly Duckling Phase” is a sign of healthy development. Rather than rushing into treatment, embrace this natural stage and trust the process—your child’s perfect smile is likely already in motion.

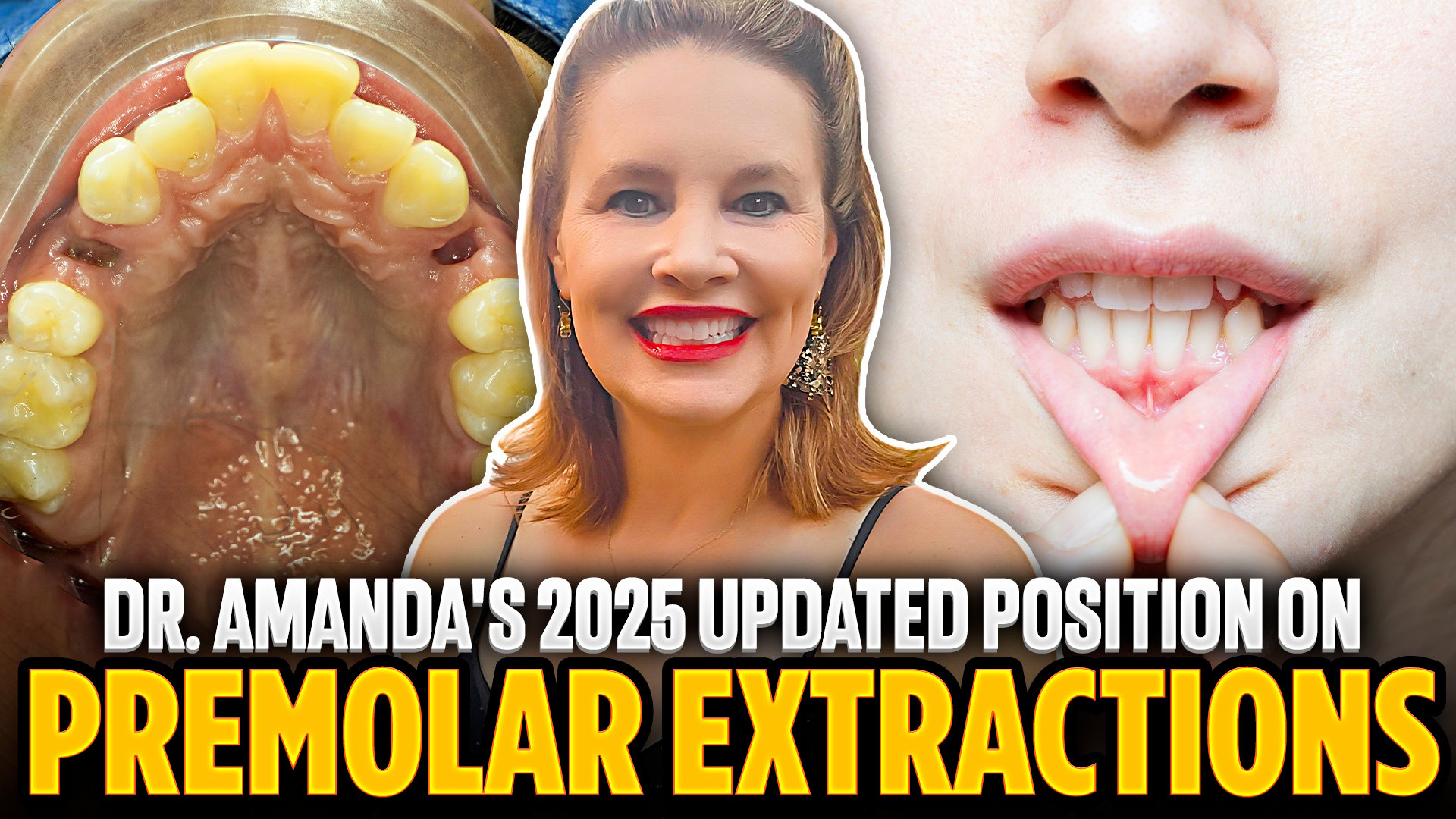
Dr. Amanda’s Position on Premolar Extractions- 2025 for Braces and Invisalign
Dr. Amanda’s Position on Premolar Extractions- 2025 for Braces and Invisalign
- Introduction
- If you’re still automatically reaching for extractions in tough ortho cases, it might be time to reassess.
- The conversation around premolar extractions has evolved, and so should your approach.
- Whether you’re new to orthodontics or a seasoned pro, understanding when extractions are truly necessary can elevate your treatment planning.
- Rewind: Why You Might Be Over-Extracting
- Years ago, many of us were trained to extract by default—especially in crowded cases.
- You might have been taught that over 50% of patients needed extractions.
- But let’s be honest: most of those cases didn’t really need it.
- Often, it was because we missed the window for early intervention.
III. Why Early Intervention (Phase One) Changes the Game
- If you’re seeing a child early—while they’re still growing—you have more tools and options.
- Starting Phase One treatment on time can drastically reduce the need for extractions later.
- No major airway issues? No intense oral habits? Then you’re probably good to go without pulling teeth.
- Catch it early, and you can shape the arch naturally.
- When Extractions Are Still on the Table
- Sometimes, you’ll meet patients who are done growing and have limited space.
- Thin tissue biotype? Minimal bone? Non-surgical options may be limited.
- If expansion or proclination isn’t safe, extractions might still be your best route.
- Just be sure you’re not defaulting to this without exploring all your options first.
- What You Should Be Doing Now
- Use your CBCT tools (like those in the Invisalign portal) to evaluate bone and space.
- Don’t rely on guesswork—use imaging to guide decisions.
- Review your non-surgical options: arch expansion, distalization, proclination, IPR, etc.
- Not sure how to use all five methods? Go refresh with some training or tutorials.
- The Bottom Line
- Stop treating all cases the same.
- Start early when you can—it’s your best shot at avoiding extractions.
- And if you must extract, do it with confidence knowing you’ve explored every alternative.
- Your patients (and their smiles) will thank you.
Dr. Amanda’s 2025 Pulse of the Orthodontic Market Forecast
Dr. Amanda’s 2025 Pulse of the Orthodontic Market Forecast
- I. Introduction
- Amanda from StraightSmile Solutions.
- Time for another market pulse update, focused on Q2 of 2025.
- Regular updates to keep orthodontic professionals informed and prepared.
- Current Market Snapshot
- Things are currently a little slow in the orthodontic industry.
- This trend aligns with broader market downturns.
- Similar to the 2008 experience: when consumers are uncertain, elective spending drops—especially for adult orthodontics.
III. The Resilient Demand: Kids’ Orthodontics
- Parents may delay but will always prioritize orthodontics for their kids.
- Even if not immediate, demand for pediatric orthodontic care remains strong and inevitable.
- Practices should focus on preparing for that steady demand.
- The Summer Surge Forecast
- Widespread consensus from podcasts, colleagues, and clients: Summer 2025 will be a boom.
- Now is the time to get practices and systems in place.
- Anticipate a rush of new patients and demand.
- Key Growth Areas to Focus On
- Phase One Orthodontics
- Early interceptive treatments for younger children.
- Early Comprehensive Cases
- Start before full adult dentition.
- Braces
- Braces are cool again, thanks to TikTok and cultural trends.
- Surge in interest, especially among teens.
- Indirect Bonding
- Some large companies may be exiting, but resources and support still available through StraightSmile Solutions.
- Invisalign First & Expanders
- Time to ramp up scanner usage.
- Get cases launched before May to ride the summer wave.
- Final Advice from Dr. Amanda
- Act now to set up your systems, staff, and supply chains.
- Market may be slow today, but preparation now = success later.
- StraightSmile Solutions is here to help every step of the way.
VII. Call to Action
- Visit StraightSmileSolutions.com for support, tips, and resources to optimize your practice for the upcoming boom.

