 I. Introduction
I. Introduction
- The Phase 1 debond checklist is completely different from the comprehensive/Phase 2.
- Many clinicians either under-bake (raw) or overdo (burnt) Phase 1.
- Poorly done Phase 1 can lead to board complaints or refund requests, especially if another provider catches the mistakes.
II. The Goal of Phase 1
- Fix the bite, habits, and myofunctional issues.
- Set up the foundation so that permanent teeth (3s, 4s, 5s, 7s) have space to erupt.
- No guarantees that every tooth will come in perfectly, but you must create the space.
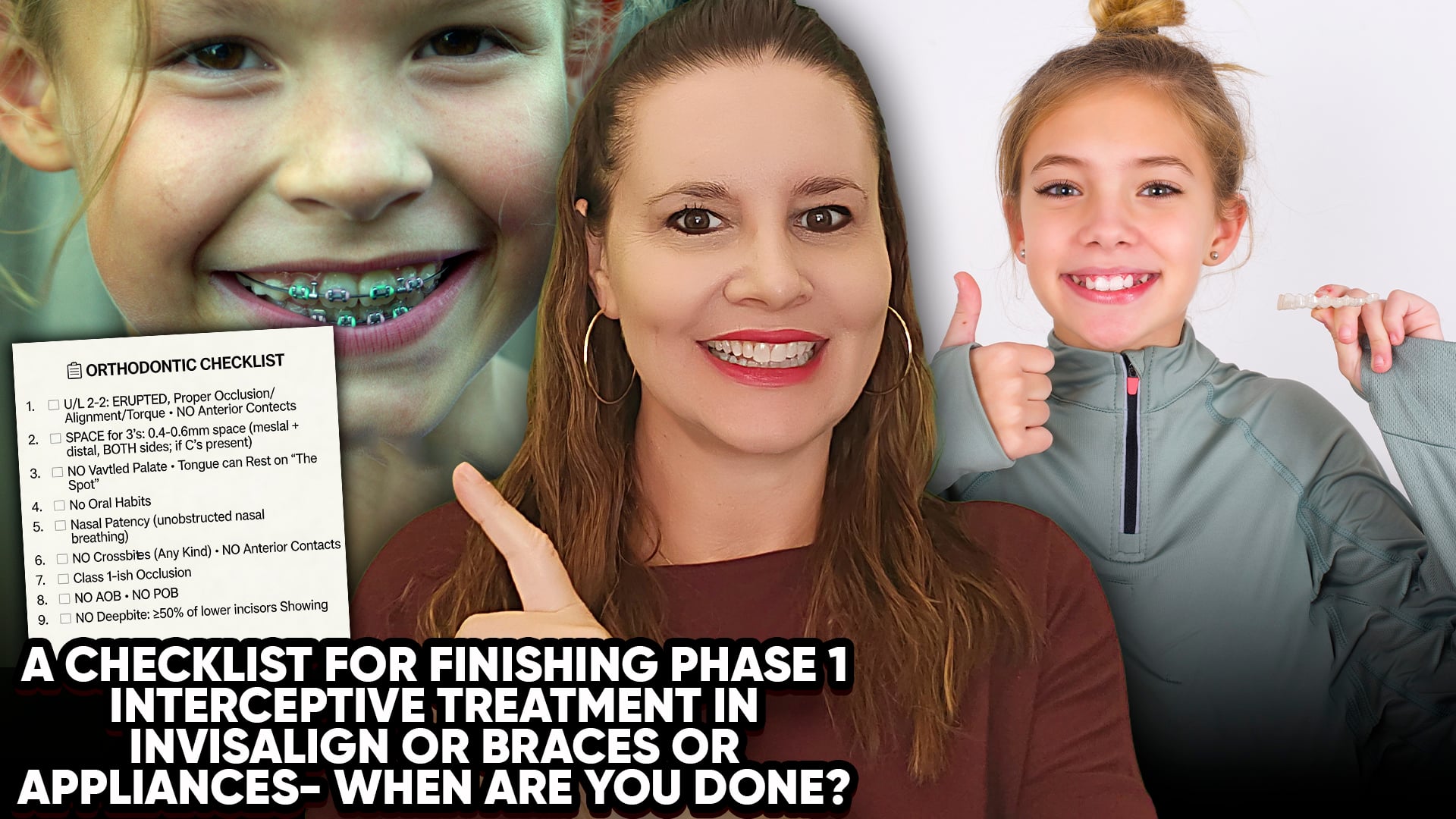
III. The Debond Checklist
- Upper and lower 2-2 (7-10) should be erupted, aligned, and in proper occlusion.
- There should be a small overjet – no anterior tooth-to-tooth contact.
- If Cs (canine primary teeth) are still present, there must be space around them for the permanent canines.
- No vaulted palate – palate should be remodelled (RPE or IPE done).
- No crossbites (anterior or posterior). The upper arch should be about half a tooth wider than the lower.
- No crowding. Over-expand rather than under-expand extra space is fine.
- No anterior open bite (AOB) or posterior open bite (POB). Back teeth should touch.
- Vertical overlap: see 10-60% of lower incisors – no deep bite.
- Nasal patency and oral habits must be addressed (myo/ENT clearance obtained before starting).
IV. The Retention and Recall Period
- Retention after Phase 1 is often unnecessary – children outgrow retainers quickly.
- Have upfront conversations about what is included (retainers, recalls).
- Keep patients on tight recall every 3 – 6 months between Phase 1 and Phase 2 – these visits are included in the fee, so charge appropriately.
- Good recall keeps patients from going elsewhere for Phase 2.
V. The Bottom Line
- Phase 1 is done when the bite is corrected, space is created, and airway/myo issues are managed.
- Document everything. Get specialist clearances in writing.
- Don’t rush. A proper Phase 1 prevents liability and makes Phase 2 easy.