Open Mouth Posture in Cephs – Numbers Invalid? Turning CBCT into Cephs with Extension Arms
I. Introduction
Dr. Amanda explains how open mouth posture during cephalometric imaging leads to invalid or distorted measurements, particularly when converting CBCT scans to 2D cephs. As more clinicians adopt CBCT extension arms or outsource ceph conversions, understanding proper mouth closure protocols becomes critical for diagnostic accuracy. She emphasizes establishing a consistent workflow and verifying patient posture before image capture.
- Ceph Workflow and Equipment Setup
- Clinicians may use CBCT machines with extension arms or services like Beam Readers and 3DX to extract ceph images.
B. Dr. Amanda stresses the need to practice image acquisition before complex cases arise.
C. Each CBCT system differs in setup; clinicians should consult manufacturers for proper bite positioning tools and calibration settings.
III. Importance of Mouth Closure
- The mouth must be fully shut for accurate skeletal and dental relationships.
B. If “daylight” (visible space) is seen between both anterior and posterior teeth, the ceph is invalid.
C. Open-mouth posture skews mandibular readings, causing diagnostic errors in Class II or III evaluation. - Impact on Cephalometric Measurements
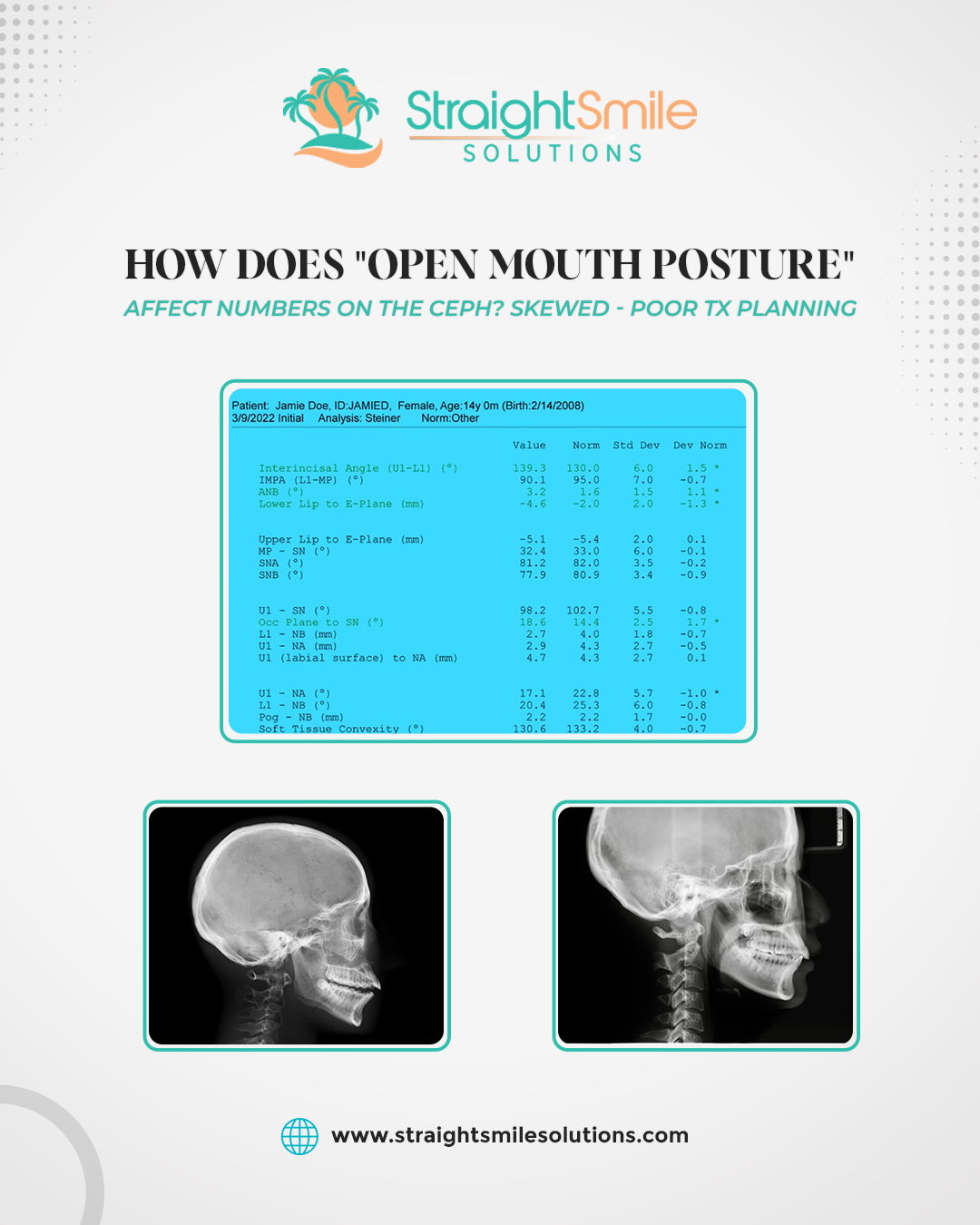
- Accurate values: SNA angle, upper incisor to NA, and maxillary metrics remain reliable.
B. Distorted values: SNB, ANB, mandibular position, and vertical skeletal dimensions.
C. An open mouth alters the hinge position of the mandible, lengthening facial height artificially. - Case Example and Clinical Insight
- In a Phase I case showing a possible Class III profile, ceph readings were misleading due to an open-mouth posture.
B. True diagnosis revealed a retrognathic maxilla (small SNA) rather than a prognathic mandible.
C. This highlights the importance of reviewing ceph posture before interpretation. - Clinical Recommendations
- Always confirm bite closure prior to scanning.
B. Request retakes if an imaging center returns open-mouth cephs; no patient should be recharged.
C. Develop internal standard protocols for CEPH imaging and posture verification.
VII. Conclusion
Open mouth posture compromises cephalometric reliability by distorting mandibular and interjaw measurements. While some maxillary readings remain usable, skeletal analysis becomes invalid for treatment planning. Clinicians must ensure proper bite closure, equipment calibration, and staff training to produce accurate cephs. Maintaining image quality protects diagnostic confidence, prevents re-radiation, and enhances orthodontic outcomes.